Top Videos
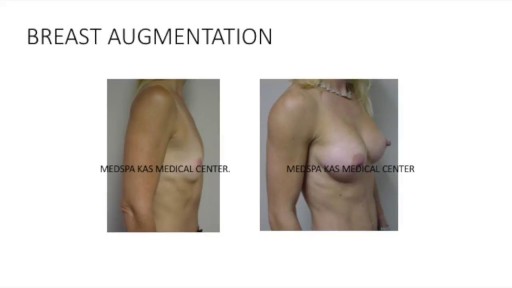
This is a complete video of breast augmentation procedure with implants also includes some before after photographs of breast augmentation surgery by Dr. Ajaya Kashyap at MedSpa Clinic, Delhi, India. source: https://www.youtube.com/watch?v=tRg3RkvCvOE Get more information: www.bestbreastsurgeryindia.com Get more information: www.themedspa.us Email at: info@themedspa.us Call/WhatsApp on:+91-9818369662, 9958221983/82/81

Huge Ovarian Cyst Removal From 85 Years Old Woman.

TV interview with Dr. Mostafa Yakoot, MD discussing his recently published study for efficacy of lettuce seed oil in patients with insomnia

An esophageal stent is a flexible mesh tube, approximately 2cm (3/4 inch) wide, and is placed through the constricted area of your esophagus (food tube) to allow food and beverages to pass from your mouth to your stomach for digestion and absorption of nutrients.


The pain of ovulation can range from a mild twinge to severe discomfort and usually lasts from minutes to hours. It is generally felt on one side of the abdomen and may vary each month, depending on which ovary is releasing the egg during that cycle.
Que Es Bueno Para La Diabetes Medicina Natural. Porque Con Este Método Que Voy a Revelarte que es 10 Veces Más Efectivo Que Cualquier Otro Podrás Vencer A Tu Diabetes RÁPIDAMENTE. Si no hubiera sido por el poderoso método inusual pero PROBADO que usé para obtener RESULTADOS rápidos y controlar la diabetes. La genialidad de este gran descubrimiento es que está diseñado para controlar, frenar y vencer a la diabetes. con la “complicidad” de tu propio cuerpo que se auto regenera si se le instalan los comando correctos en el metabolismo. Sin importar si tienes 7 ó 90 años. Sin importar si tu nivel de azúcar es más incontrolable que un caballo salvaje, o tu tipo de diabetes. Sin importar cuantas veces tu doctor te ha dicho que la diabetes no tiene cura. Sin importar si has fallado una docena de veces con tratamientos, medicamentos o métodos convencionales que NO SIRVEN. Estás a punto de descubrir cómo controlar la diabetes usando la Solución Natural más exitosa jamás revelada que transformará tu cuerpo en una máquina generadora de salud y energía – ¡en tan solo unos pocos días! haciendo click aqui. http://vencer-la-diabetes-rapido.info-pro.co

Bizarre Body Modifications

http://www.landging.com/accident-animation-workers-compensation-lifting-box.html
This lifting box accident animation demonstrates the injury covered by workers compensation program.

Twin Childbirth Video

Henry Anhalt DO FAAP
Ped Eddo
How teeth braces are put


A video showing the process of childbirth via vaginal delivery.

Watch that video to know the Natural Ways to Whiten Teeth at Home

Examination of the knee joint from the USMLE collection

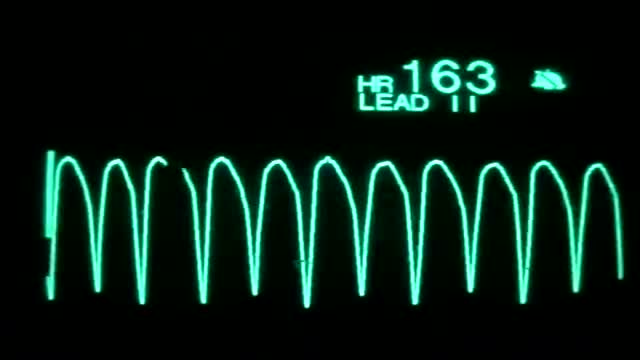
On the rhythm strip, the QRS might be somewhat taller or wider. One commonly seen type of polymorphic ventricular tachycardia is torsades de pointes. Torsades and other polymorphic VT are advanced rhythms which require additional expertise and expert consultation is advised.

A new video illustrating the horizontal breast exam technique whihc is performed by doctors for any breast masses or abnormalities.

