- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Cataract Surgery is a brief outpatient surgery. Done with modern advancements it reqires no stitches, no patches or no needles. It is done on an outpatient basis at http://redrocksurgerycenter.com by Drs. David Malitz and Dr. Surjeet Singh in Las Vegas, Nevada. Althouth the procedure is brief, there are risks, alternatives benefits and potential complications. To minimize these adverse effects, pick an experienced Surgeon. Just call 702-509-1733 for a FREE screening or visit http://sweyeinstitute.com. With our modern implants you can even reduce or eliminate your need for glasses after surgery! It is your eyes, it is worth the trip, most insurance accepted and uninsured patients are no problem!
A disease of the immune system due to infection with HIV. HIV destroys the CD4 T lymphocytes (CD4 cells) of the immune system, leaving the body vulnerable to life-threatening infections and cancers. Acquired immunodeficiency syndrome (AIDS) is the most advanced stage of HIV infection. To be diagnosed with AIDS, a person with HIV must have an AIDS-defining condition or have a CD4 count less than 200 cells/mm³ (regardless of whether the person has an AIDS-defining condition).

Dialysis services at UC San Diego Health: https://health.ucsd.edu/care/kidney/dialysis
UC San Diego Health Licensed Clinical Social Worker, Norma Reggev, discusses hemodialysis as a treatment option for failing kidneys with patient testimonials. Discussion includes In Center Hemodialysis and Home Hemodialysis.
0:00 - Hemodialysis
1:34 - When Should Dialysis Begin?
2:00 - What is Dialysis?
2:25 - How Hemodialysis Works
3:15 - In-Center Hemodialysis Considerations
3:42 - Patient Shares Their Experience With In-Center Hemodialysis
7:30 - Home Hemodialysis Considerations
8:35 - Patient Shares Their Experience With Home Hemodialysis
12:23 - Types of Vascular Access
Central Line Placement

How To Breastfeed - Deep Latch Technique
Multiple myeloma is a cancer that affects plasma cells, a kind of white blood cell found in the soft insides of your bones, called marrow. Plasma cells are part of your body's immune system. They make antibodies to help fight off infections.

Verrugas En El Cuello, Como Borrar Lunares De La Cara, Como Quitar Las Verrugas Del Cuello --- http://sinverrugasylunares.plus101.com --- El Ajo Para Eliminar Las Verrugas, PRUEBALO!!! Antes que nada déjame comentarte que el ajo es un poderoso antiséptico, con propiedades fungicidas, bactericidas y también ayudan a depurar nuestro cuerpo. El ajo es rico en un compuesto llamado alicina, este elemento es un poderoso antivirus y anti bacterial natural, eso sin mencionar las propiedades antioxidantes que el ajo posee las cuales son de enorme beneficio para la salud de nuestra piel y por supuesto la salud en general. Es un tratamiento sencillo pero bastante efectivo, te recomiendo que lo comiences a partir de hoy mismo. Por las mañanas en ayunas tomate un ajo crudo, esto con el fin de limpiar nuestro organismo de virus y bacterias. Recuerda que nuestra misión es eliminar la raíz de las verrugas y los lunares tal como lo hablamos anteriormente el responsable de las verrugas es el virus del papiloma humano. El ajo gracias a sus propiedades antivirales nos ayudarán a combatir el virus desde adentro. Haz esto todos los días. Tomándote un ajo diario en ayunas estarás atacando el virus desde adentro, Ahora lo atacaremos desde fuera Para esto necesitarás un ajo, debes partirlo en porciones pequeñas calcula el tamaño de las porciones para cubrir los lunares y/o tus verrugas. Y ahora da a conocer el mismo método que él utilizó para curarse y eliminar las verrugas y lunares para siempre. Te invito a conocerlo a través del siguiente enlace: http://sinverrugasylunares.plus101.com
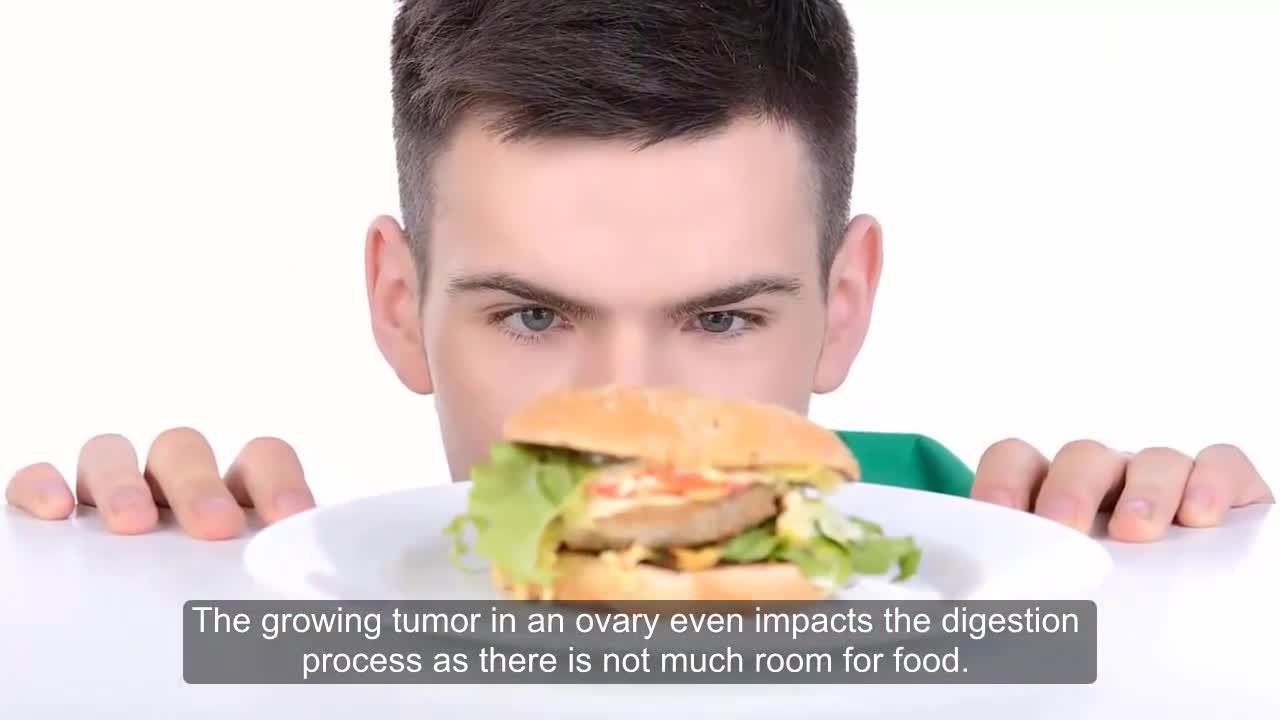
Ovarian cancer warning signs include ongoing pain or cramps in the belly or back, abnormal vaginal bleeding, nausea, and bloating. Depending on the cancer stage, ovarian cancer treatment includes surgery and chemotherapy.

In this video, Dr. Robert Rozbruch, chief of Limb Lengthening and Complex Reconstruction at Hospital for Special Surgery performs an osseointegration after a primary amputation. The patient, a 40 year old woman, had chronic nerve pain and compromised function of her residual limb.
For more information, visit: https://www.limblengthening.com/
https://www.hss.edu/limblengthening
https://www.hss.edu/LSARC
https://www.facebook.com/limblengtheningNYC
https://www.instagram.com/limblengthening
https://www.twitter.com/limblengthen
https://www.youtube.com/channe....l/UC-JL_X6ALjZXiXtcP
key words: Osseointegration, Amputee, Amputation, Limb Replacement, Tibia, Osseointegration

DMC Surgeon uses minimally-invasive surgery to remove uterine fibroids to hasten recovery. ~ Detroit Medical Center

Educational video of male patient receiving an anoscopy.

Full examination of the female from head to toe by Loyola Medical School, Chicago. Part 3

An African traditional healer performing a brain surgery.

Wow! Ultrasound guided internal jugular vein cannulation (long axis approach)

A spontaneous vaginal delivery (SVD) occurs when a pregnant woman goes into labor with or without use of drugs or techniques to induce labor, and delivers her baby in the normal manner, without forceps, vacuum extraction, or a cesarean section. Assisted vaginal delivery (AVD) occurs when a pregnant woman goes into labor with or without the use of drugs or techniques to induce labor, and requires the use of special instruments such as forceps or a vacuum extractor to deliver her baby vaginally.

This video: Patent ductus arteriosus (PDA) is a persistent opening between two major blood vessels leading from the heart. The opening, called the ductus arteriosus, is a normal part of a baby's circulatory system before birth that usually closes shortly after birth. If it remains open, however, it's called a patent ductus arteriosus. A small patent ductus arteriosus often doesn't cause problems and might never need treatment. However, a large patent ductus arteriosus left untreated can allow poorly oxygenated blood to flow in the wrong direction, weakening the heart muscle and causing heart failure and other complications. Treatment options for a patent ductus arteriosus include monitoring, medications and closure by cardiac catheterization or surgery.

An esophageal stent is a flexible mesh tube, approximately 2cm (3/4 inch) wide, and is placed through the constricted area of your esophagus (food tube) to allow food and beverages to pass from your mouth to your stomach for digestion and absorption of nutrients.

Endoscopic finding in a patient with a typical rectal cancer (adenocarcinoma)

TV interview with Dr. Mostafa Yakoot, MD discussing his recently published study for efficacy of lettuce seed oil in patients with insomnia
