I migliori video
Thrombotic thrombocytopenic purpura (TTP) is a rare blood disorder characterized by clotting in small blood vessels of the body (thromboses), resulting in a low platelet count. In its full-blown form, the disease consists of the pentad of microangiopathic hemolytic anemia, thrombocytopenic purpura, neurologic abnormalities, fever, and renal disease
Cirrhosis is a late stage of scarring (fibrosis) of the liver caused by many forms of liver diseases and conditions, such as hepatitis and chronic alcoholism. The liver carries out several necessary functions, including detoxifying harmful substances in your body, cleaning your blood and making vital nutrients. Cirrhosis occurs in response to damage to your liver. Each time your liver is injured, it tries to repair itself. In the process, scar tissue forms. As cirrhosis progresses, more and more scar tissue forms, making it difficult for the liver to function. Decompensated cirrhosis is the term used to describe the development of specific complications resulting from the changes brought on by cirrhosis. Decompensated cirrhosis is life-threatening. The liver damage done by cirrhosis generally can't be undone. But if liver cirrhosis is diagnosed early and the cause is treated, further damage can be limited and, rarely, reversed.
To identify an UTI, keep an eye out for the following symptoms: A burning feeling when you urinate. A frequent or intense urge to urinate, even though little comes out when you do. Pain or pressure in your back or lower abdomen. Cloudy, dark, bloody, or strange-smelling urine. Feeling tired or shaky.

Tendons are thick cords that join your muscles to your bones. When these tendons become irritated or inflamed, it is called tendinitis. This condition causes acute pain and tenderness, making it difficult to move the affected joint. Read more

A colostomy is an operation that creates an opening for the colon, or large intestine, through the abdomen. A colostomy may be temporary or permanent. It is usually done after bowel surgery or injury.

How to Use Wash your hands. Check the drug label to be sure it is what your doctor prescribed. ... Remove pen cap. Look at the insulin. Wipe the tip of the pen where the needle will attach with an alcohol swab or a cotton ball moistened with alcohol.
Fulminant hepatic failure (FHF) or acute liver failure (ALF) is defined as the rapid development of acute liver injury with severe impairment of the synthetic function and hepatic encephalopathy in a patient without obvious, previous liver disease.
Function. Vitamin A helps form and maintain healthy skin, teeth, skeletal and soft tissue, mucus membranes, and skin. It is also known as retinol because it produces the pigments in the retina of the eye. Vitamin A promotes good vision, especially in low light. Vitamin deficiency anemia occurs when your body doesn't have enough of the vitamins needed to produce adequate numbers of healthy red blood cells. Red blood cells carry oxygen from your lungs throughout your body. If your diet is lacking in certain vitamins, vitamin deficiency anemia can develop.
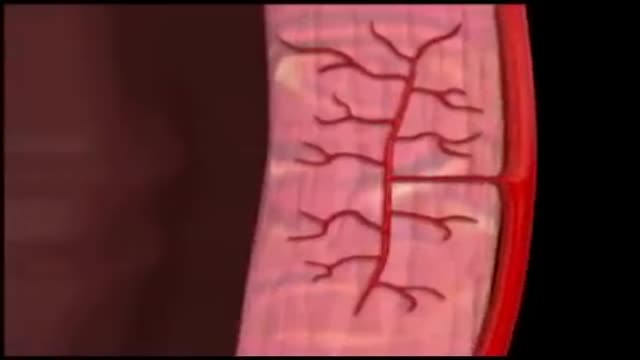
Coronary circulation is the circulation of blood in the blood vessels of the heart muscle (myocardium). The vessels that deliver oxygen-rich blood to the myocardium are known as coronary arteries. The vessels that remove the deoxygenated blood from the heart muscle are known as cardiac veins.
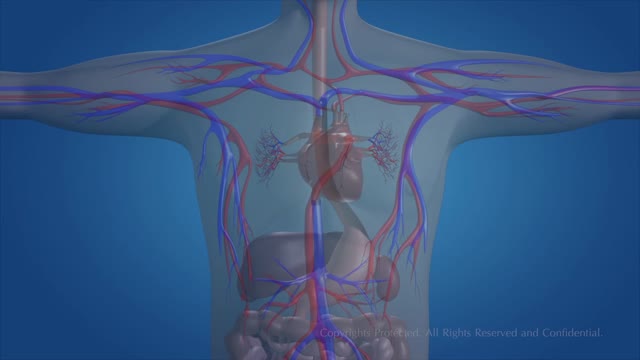
The essential components of the human cardiovascular system are the heart, blood and blood vessels. It includes the pulmonary circulation, a "loop" through the lungs where blood is oxygenated; and the systemic circulation, a "loop" through the rest of the body to provide oxygenated blood.

To remove a smaller stone in your ureter or kidney, your doctor may pass a thin lighted tube (ureteroscope) equipped with a camera through your urethra and bladder to your ureter. Once the stone is located, special tools can snare the stone or break it into pieces that will pass in your urine.

Fibromyalgia syndrome (FMS) is a form of fibromyalgia where pain and stiffness occurs in muscles, tendons, and ligaments throughout the body, accompanied by other generalized symptoms such as fatigue, sleep disruption or unrefreshing sleep, mood disorder, and cognitive difficulties such as poor memory or mental ...
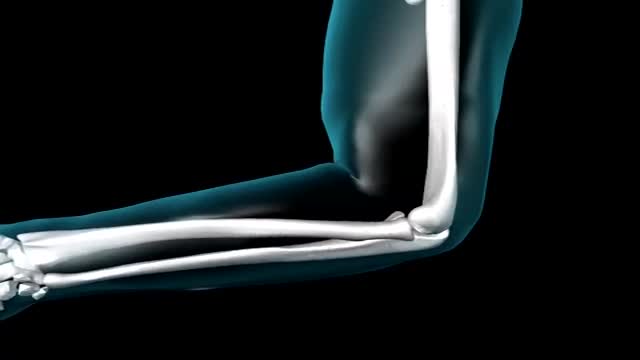
Elbow. In primates, including humans, the elbow joint is the synovial hinge joint between the humerus in the upper arm and the radius and ulna in the forearm which allows the hand to be moved towards and away from the body.

The easy experimental answer to this question is 264 hours (about 11 days). In 1965, Randy Gardner, a 17-year-old high school student, set this apparent world-record for a science fair. Several other normal research subjects have remained awake for eight to 10 days in carefully monitored experiments. None of these individuals experienced serious medical, neurological, physiological or psychiatric problems. On the other hand, all of them showed progressive and significant deficits in concentration, motivation, perception and other higher mental processes as the duration of sleep deprivation increased. Nevertheless, all experimental subjects recovered to relative normality within one or two nights of recovery sleep. Other anecdotal reports describe soldiers staying awake for four days in battle, or unmedicated patients with mania going without sleep for three to four days.
Funny School Exam

Dacryocystorhinostomy (DCR) is a procedure performed for the treatment of tearing (epiphora) due to blockage of the nasolacrimal duct. Tears originate in the lacrimal gland, located at the upper outer margin of the eye. As tears cross the eye with each blink, they are directed into small openings in the eyelids called puncta. From this point, tears travel through a pathway known as the canalicular system into the lacrimal sac. The lacrimal sac is located between the eye and the nose, and funnels tears into the nasal cavity through the nasolacrimal duct (Figure 1). As this is quite a long path for tears to travel, there can be many causes of excessive tearing. Blockage of the nasolacrimal duct is one common cause, and can be treated by creating a direct opening from the lacrimal sac into the nasal cavity in a procedure known as DCR. The evaluation and management of tearing may involve both an ophthalmologist and an otolaryngologist.
An intelligence quotient (IQ) is a total score derived from one of several standardized tests designed to assess human intelligence. IQ is a number meant to measure people cognitive abilities (intelligence) in relation to their age group. An I.Q between 90 and 110 is considered average; over 120, superior. Roughly 68% of the population has an IQ between 85 and 115. The average range between 70 and 130, and represents about 95% of the population.

COMMON BLOOD DISORDERS
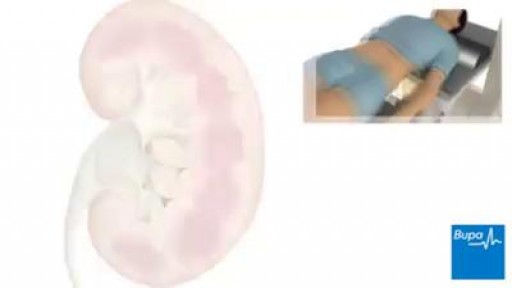
extracorporeal shockwave lithotripsy is used to treat kidney stones
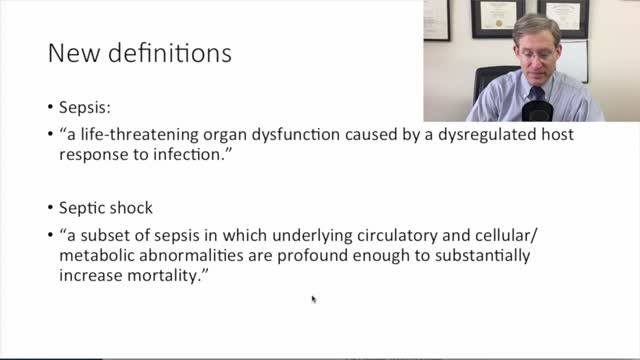
new sepsis definitions
