- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Fibromyalgia syndrome (FMS) is a form of fibromyalgia where pain and stiffness occurs in muscles, tendons, and ligaments throughout the body, accompanied by other generalized symptoms such as fatigue, sleep disruption or unrefreshing sleep, mood disorder, and cognitive difficulties such as poor memory or mental ...
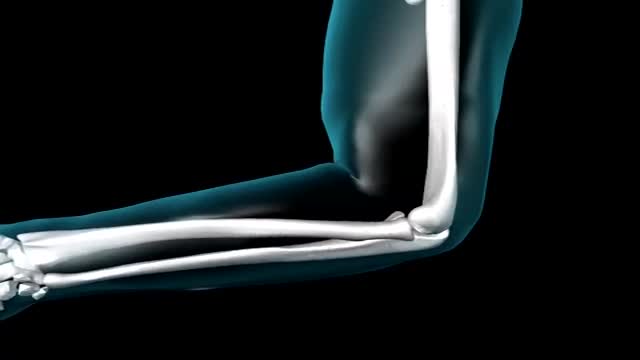
Elbow. In primates, including humans, the elbow joint is the synovial hinge joint between the humerus in the upper arm and the radius and ulna in the forearm which allows the hand to be moved towards and away from the body.

This upgraded ultrasound device allows you to see your organs with the help of augmented reality glasses

The easy experimental answer to this question is 264 hours (about 11 days). In 1965, Randy Gardner, a 17-year-old high school student, set this apparent world-record for a science fair. Several other normal research subjects have remained awake for eight to 10 days in carefully monitored experiments. None of these individuals experienced serious medical, neurological, physiological or psychiatric problems. On the other hand, all of them showed progressive and significant deficits in concentration, motivation, perception and other higher mental processes as the duration of sleep deprivation increased. Nevertheless, all experimental subjects recovered to relative normality within one or two nights of recovery sleep. Other anecdotal reports describe soldiers staying awake for four days in battle, or unmedicated patients with mania going without sleep for three to four days.
Funny School Exam

Dacryocystorhinostomy (DCR) is a procedure performed for the treatment of tearing (epiphora) due to blockage of the nasolacrimal duct. Tears originate in the lacrimal gland, located at the upper outer margin of the eye. As tears cross the eye with each blink, they are directed into small openings in the eyelids called puncta. From this point, tears travel through a pathway known as the canalicular system into the lacrimal sac. The lacrimal sac is located between the eye and the nose, and funnels tears into the nasal cavity through the nasolacrimal duct (Figure 1). As this is quite a long path for tears to travel, there can be many causes of excessive tearing. Blockage of the nasolacrimal duct is one common cause, and can be treated by creating a direct opening from the lacrimal sac into the nasal cavity in a procedure known as DCR. The evaluation and management of tearing may involve both an ophthalmologist and an otolaryngologist.
An intelligence quotient (IQ) is a total score derived from one of several standardized tests designed to assess human intelligence. IQ is a number meant to measure people cognitive abilities (intelligence) in relation to their age group. An I.Q between 90 and 110 is considered average; over 120, superior. Roughly 68% of the population has an IQ between 85 and 115. The average range between 70 and 130, and represents about 95% of the population.
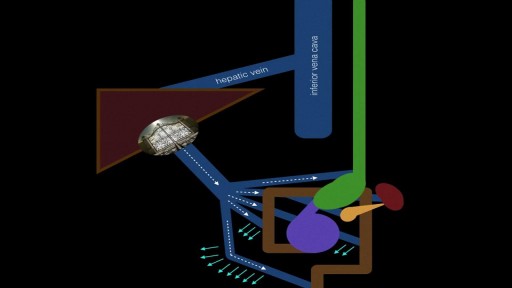
Portal hypertension is an increase in the blood pressure within a system of veins called the portal venous system. ... If the vessels in the liver are blocked due to liver damage, blood cannot flow properly through the liver. As a result, high pressure in the portal system develops

COMMON BLOOD DISORDERS

Michigan Medicine’s Cardiac Surgery Simplified series highlights a multitude of surgical procedures in order to educate patients, healthcare providers, and trainees interested in learning about cardiac surgery performed at the Frankel Cardiovascular Center.
Like and subscribe to our channel to learn more about our pioneering procedures including minimally invasive valve surgery and safer methods to repair aortic aneurysms and dissections.
To learn more about cardiac surgery at Michigan Medicine, visit: https://medicine.umich.edu/dept/cardiac-surgery
To learn more about Frankel Cardiovascular Center, visit: https://www.umcvc.org/
To watch the full playlist, visit: https://www.youtube.com/playli....st?list=PLNxqP-XbH8B
-------------------------------------------------------
Subscribe to Michigan Medicine’s YouTube channel for upcoming videos and future live streams featuring our experts answering your questions.
-------------------------------------------------------
Follow Michigan Medicine on Social:
Twitter: https://twitter.com/umichmedicine
Instagram: https://www.instagram.com/umichmedicine/
Facebook: https://www.facebook.com/MichiganMedi...
Follow the U-M Frankel Cardiovascular Center on Social:
Twitter: https://twitter.com/umichcvc
Facebook: https://www.facebook.com/Universityof...
#MichiganMedicine #MedEd #CardiacSurgery #UniversityOfMichiganHealth #FrankelCardiovascularCenter #Cardiology
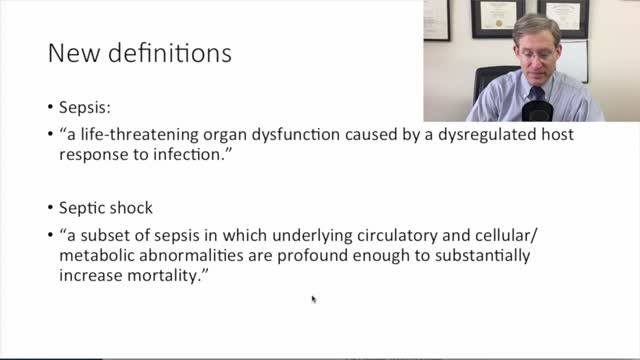
new sepsis definitions
Learn about Bicuspid Aortic Valves in this presentation. Bicuspid Aortic Valves are present in about 2% of the population and are the most common congenital disorder. Find out more about a Bicuspid Aortic Valve by visiting the following link:
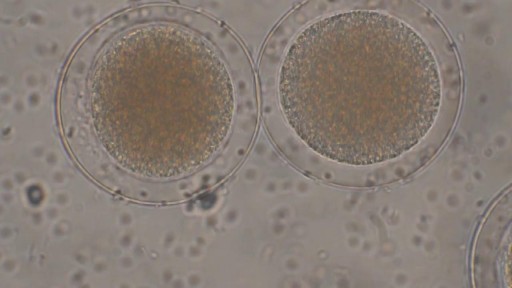
Sperm Meets Egg: Weeks 1 to 3 of Pregnancy. Something magical is about to happen! Watch as the ovulation process occurs, and then millions of sperm swim upstream on a quest to fertilize an egg. Your due date is calculated from the first day of your last menstrual period

Spontaneous pneumothorax is a life-threatening condition in patients with severe underlying lung disease; thus, tube thoracostomy is the procedure of choice in SSP. Pleurodesis decreases the risk of recurrence, as does thoracotomy or video-assisted thoracoscopic surgery (VATS) to excise the bullae
Antiphospholipid (AN-te-fos-fo-LIP-id) syndrome occurs when your immune system attacks some of the normal proteins in your blood. It can cause blood clots in your arteries or veins. And it can cause pregnancy complications, such as miscarriage and stillbirth. Blood clots in your leg veins cause a condition known as deep vein thrombosis (DVT). Damage from blood clots in your organs, such as your kidneys, lungs or brain, depends on the extent and location of the clot. For instance, a clot in your brain can cause a stroke. There's no cure for antiphospholipid syndrome, but medications can reduce your risk of blood clots.

The hepatitis A virus, which causes the infection, usually is spread when a person ingests even tiny amounts of contaminated fecal matter. The hepatitis A virus infects liver cells and causes inflammation. The inflammation can impair liver function and cause other signs and symptoms of hepatitis A. Hepatitis A virus can be transmitted several ways, such as: Eating food handled by someone with the virus who doesn't thoroughly wash his or her hands after using the toilet Drinking contaminated water Eating raw shellfish from water polluted with sewage Being in close contact with a person who's infected — even if that person has no signs or symptoms Having sex with someone who has the virus

There is any chance that the snake is venomous The person has difficulty breathing There is loss of consciousness If you know the snake is not venomous, treat as a puncture wound. 1. Note the Snake's Appearance Be ready to describe the snake to emergency staff. 2. Protect the Person While waiting for medical help: Move the person beyond striking distance of the snake. Have the person lie down with wound below the heart. Keep the person calm and at rest, remaining as still as possible to keep venom from spreading. Cover the wound with loose, sterile bandage. Remove any jewelry from the area that was bitten. Remove shoes if the leg or foot was bitten. Do not: Cut a bite wound Attempt to suck out venom Apply tourniquet, ice, or water Give the person alcohol or caffeinated drinks or any other medications
Treatment of periodontal disease - Scaling and root planing
Disc Disease Videos Watch Disc Disease Videos There are several symptoms that are fairly consistent for people with lower back pain or neck pain from degenerative disc disease, including: Pain that is usually related to activity and will flare up at times but then return to a low-grade pain level, or the pain will go away entirely The amount of chronic pain—referred to as the patient's baseline level of pain—is quite variable between individuals and can range from almost no pain/just a nagging level of irritation, to severe and disabling pain Severe episodes of back or neck pain that will generally last from a few days to a few months before returning to the individual's baseline level of chronic pain Chronic pain that is completely disabling from degenerative disc disease does happen in some cases, but is relatively rare See Treating Chronic Pain and Depression from Degenerative Disc Disease
