- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

The complex circuitry interconnecting different areas in the brain, known collectively as white matter, is composed of millions of axons organized into fascicles and bundles. Upon macroscopic examination of sections of the brain, it is difficult to discern the orientation of the fibers. The same is true for conventional imaging modalities. However, recent advancements in magnetic resonance imaging (MRI) make such task possible in a live subject. By sensitizing an otherwise typical MRI sequence to the diffusion of water molecules it is possible to measure their diffusion coefficient in a given direction1. Normally, the axonal membrane and myelin sheaths pose barriers to the movement of water molecules and, thus, they diffuse preferentially along the axon2. Therefore, the direction of white matter bundles can be elucidated by determining the principal diffusivity of water. The three-dimensional representation of the diffusion coefficient can be given by a tensor and its mathematical decomposition provides the direction of the tracts3; this MRI technique is known as diffusion tensor imaging (DTI). By connecting the information acquired with DTI, three-dimensional depictions of white matter fascicles are obtained4. The virtual dissection of white matter bundles is rapidly becoming a valuable tool in clinical research.
Our journey begins with a transverse section of tightly packed axons as seen through light microscopy. Although represented as a two-dimensional "slice", we see that these axons in fact resemble tubes. A simulation of water molecules diffusing randomly inside the axons demonstrates how the membranes and myelin hinder their movement across them and shows the preferred diffusion direction --along the axons. The tracts depicted through DTI slowly blend in and we ride along with them. As we zoom out even more, we realize that it is a portion of the corpus callosum connecting the two sides of the brain we were traveling on and the great difference in relative scale of the individual axons becomes evident. The surface of the brain is then shown, as well as the rest of the white matter bundles--a big, apparently chaotic tangle of wires. Finally, the skin covers the brain.
With the exception of the simulated water molecules, all the data presented in the animation is obtained through microscopy and MRI. Computer algorithms for the extraction of the cerebral structures and a custom-built graphics engine make our journey through the brain's anatomy possible in a living person.
Micrograph courtesy of Dr. Christian Beaulieu, University of Alberta.
Music by Mario Mattioli.
References:
1. Stejskal, E.O., et al., J. Chem. Phys., 1965. 42:
2. Beaulieu, C., NMR Biomed., 2002. 15:435-55.
3. Basser, P.J., et al., J. Magn. Reson. B, 1994. 103:247-54.
4. Mori, S., et al., NMR Biomed., 2002. 15:468-80.

Superficial Palpation of the Abdomen

Liposuction for weight loss with Abdominoplasty and Body Lifting
Diagnose an abusive relationship and you will be on your way to ending domestic abuse. Getting a definitive, objective diagnosis can put you in the "stop-guessing" mode and into the "start-treating" mode in moments.

Laparoscopic repair of incisional hernia

Hip replacement is a surgical procedure in which the hip joint is replaced by a prosthetic implant, that is, a hip prosthesis. Hip replacement surgery can be performed as a total replacement or a hemi replacement

Hip Replacement Surgery
LASIK Eye Surgery 3D Animation

Ingrown Toenail Surgery HD

Total Knee Replacement Surgery Video


Let SightMD walk you through an entire LASIK procedure.
Find out more about LASIK at SightMD - https://www.sightmd.com/eye-do....ctor/lasik-eye-surge

Histology of GastroEsophageal Junction
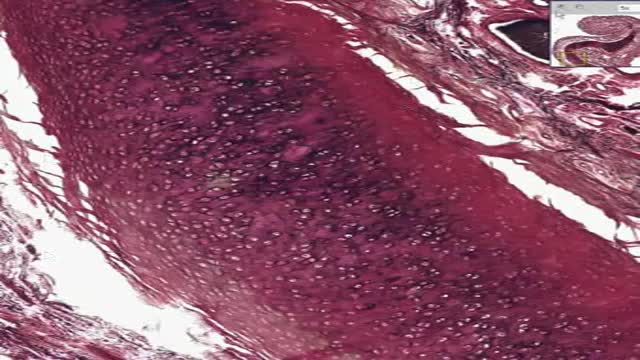
Histology of Elastic Cartilage

Shoulder dystocia is a rare emergency that can happen during the end of the second stage of labour. It's all to do with how your baby moves down through your vagina and out into the world. Shoulder dystocia happens when your baby's head has been born, but one of her shoulders becomes stuck.

Purchase a license to download a non-watermarked copy of this video here: https://www.alilamedicalmedia.....com/-/galleries/all-
Voice by: Sue Stern.
©Alila Medical Media. All rights reserved.
Support us on Patreon and get FREE downloads and other great rewards: patreon.com/AlilaMedicalMedia
Perfect for patient education purposes.
All images/videos by Alila Medical Media are for information purposes ONLY and are NOT intended to replace professional medical advice, diagnosis or treatment. Always seek the advice of a qualified healthcare provider with any questions you may have regarding a medical condition.
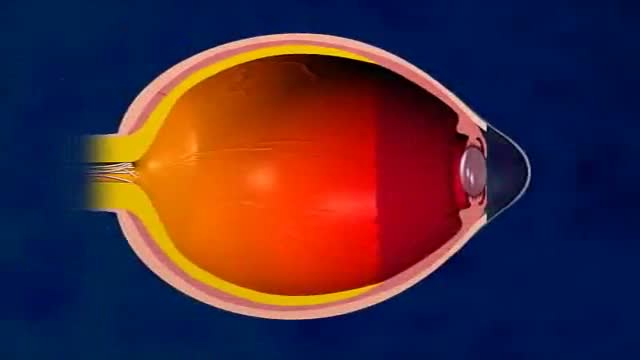
LASIK, or "laser-assisted in situ keratomileusis," is the most commonly performed laser eye surgery to treat myopia, hyperopia and astigmatism. The goal of the treatment is to reshape the cornea to correct the refractive error of the eye.
The cornea is the transparent dome-shaped structure in front of the eye. The cornea refracts light and accounts for about two-thirds of the eye's total optical power. Altering the curvature of the cornea changes the way light rays enter the eye. As a result, the light rays can be focused properly onto the retina for clearer vision.
For nearsighted people, the laser is used to flatten the cornea. For farsighted people, the cornea is made steeper. For patients with astigmatism, the laser is used to smooth the irregularly-shaped cornea into a more regular shape.
The outer layer of the cornea - the epithelium – is capable of replacing itself within a few days after being damaged or removed. The deeper layer of the cornea – the stroma, on the contrary, is a permanent corneal tissue with very limited regenerative capacity. The stroma, if reshaped by a laser, will remain that way permanently.
In this procedure, a thin, circular "FLAP" is created in the surface of the cornea to gain access to the permanent corneal tissue. This can be done with a mechanical cutting tool called a microkeratome, OR, for a blade-free experience, by a femtosecond laser. An excimer laser is then used to remove some corneal tissue to reshape the cornea. Excimer laser uses cool ultraviolet light beams to vaporize microscopic amounts of tissue in a precise manner to accurately reshape the cornea. The excimer laser is computer-controlled and is programmed based on the patient’s refractive error. The flap is then laid back in place and is allowed to heal.
LASIK eye surgery is mostly painless and can be completed within minutes. Improved vision can usually be seen overnight.
PRK, or photorefractive keratectomy, was the first type of laser eye surgery for vision correction and is the predecessor to the popular LASIK procedure. In PRK, NO flap is created. Rather, the epithelial cells on the eye surface are simply removed. An excimer laser is then used to reshape the cornea just like it does in LASIK.
The vision correction outcomes of PRK surgery are comparable to those of LASIK, but the recovery period is longer. This is because the epithelium is completely removed in PRK and it takes a few days to regenerate. PRK patients also have more discomfort and haziness of vision in the first few days after the surgery. Improved vision also takes longer to achieve.
PRK does, however, offer certain advantages. Because PRK does not involve creation of a flap, which contains both epithelial and deeper stromal tissue, the entire thickness of the stroma is available for treatment. The treatment range is therefore higher. This is particularly useful for patients with high levels of myopia or for those whose cornea is too thin for LASIK. PRK is also free of flap-related complication risks.
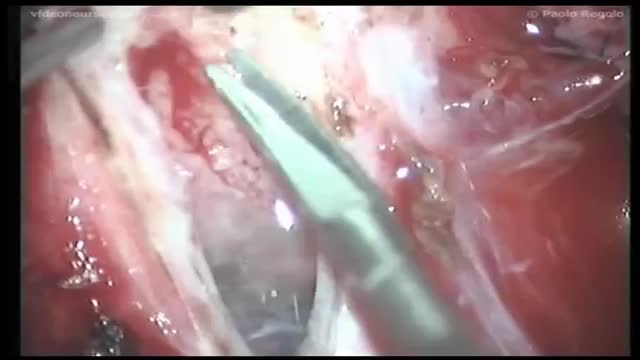
The annual incidence of primary intraspinal neoplasm is approximately five per million for females and three per million for males.[9] Spinal intradural extramedullary tumors account for two thirds of all intraspinal neoplasms and include neuromas and meningiomas.[1] Overall, meningiomas account for 25 to 46% of primary spinal neoplasms and are the second most common intradural spine tumor after neuromas.[9] Spinal meningiomas occur less frequently than intracranial ones and account for approximately 7.5 to 12.7% of all meningiomas.[25]

If you’ve suffered a sporting knee injury, how do you know when it’s serious? In this short video, Yorkshire Knee Clinic’s Dave Duffy reveals the two key tests that tell you whether your knee needs urgent, specialist attention.
𝗡𝗼𝘁𝗲𝘀 𝗳𝗼𝗿 𝘁𝗵𝗲 𝘀𝗾𝘂𝗲𝗮𝗺𝗶𝘀𝗵: This video features only features a model of the knee. There is no live footage from operations.
Discover more about sports knee injuries: https://yorkshirekneeclinic.com/sports-injuries/
Discover more about Dave Duffy: https://yorkshirekneeclinic.com/about/dave-duffy/

There are 3 major parts of the respiratory system: the airway, the lungs, and the muscles of respiration. The airway, which includes the nose, mouth, pharynx, larynx, trachea, bronchi, and bronchioles, carries air between the lungs and the body's exterior.

This Unorthodox Procedure Makes Short People A Foot Taller
