I migliori video

Position the patient with her buttocks just at the edge or just over the edge of the exam table. If she is not down far enough, inserting the speculum can be more difficult for you and uncomfortable for her.

Foley Catheter Insertion

Closing the abdomen after laparotomy

A novel technique of magnetic compression anastomosis for canalization in patients with severe biliary stricture
Acclaimed sexologist Hanny Lightfoot-Klein, author of several highly illuminating books on genital mutilation, discusses compromises in orgasm after male circumcision. Also commenting is cultural anthropologist James De Meo.From the groundbreaking documentary film, "Whose Body, Whose Rights?"

Neck and Cardiac Exam

Physical exam by a urologist including kidney, testicular and prostate exam.

Physical Examination of the abdomen

Dr. Daniel Del Vecchio, Harvard trained plastic surgeon, performs his breast lift technique, filling the upper portion of the breast for added volume
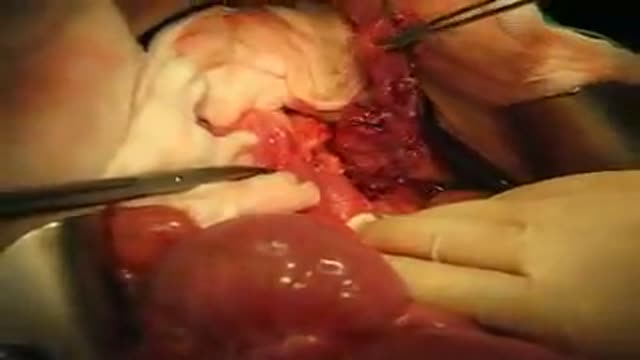
Surgery during a Pancreatectomy. One can see the pancreas half extracted. This is Experimental Surgery, taken during a Pancreas transplantation

Adult CPR video showing how to perform the Cardio-Pulmonary Resuscitation.

How to deal with heart attack and with stroke

A 30 YEAR WOMEN WITH INTRACTABLE BILIARY COLIC CASE REPORT: This 30 year women developed severe pain right upper quadrant for last 10 days. She sought many consultations and was given intravenous analgesics both (nonnarcortic and narcotic). Pain did not subside and she sought my consultation. Examination revealed her to be in agony with severe upper abdominal pain. General physical examination was otherwise unremarkable. Abdominal examination revealed mild tenderness in right hypochondrium with doubtful Murphy's sign. Urgent abdominal ultrasound showed a linear structure in bile ducts making slow writhing movements. The structure had an anechoic tube (alimentary canal) inside suggestive of a large Ascarid. Urgent ERCP was performed and bile duct and pancreatic duct cannulated selectively. Pancreatic duct was normal. Bile ducts contained a long linear filling defect extending from lower end of common bile duct to right intrahepatic duct (see image gallery for ERCP plate). A basket was introduced in the duct (see video clip) and the linear structure was engaged with soft closure and extracted out of the bile duct. Accompanying the basket was a 25 cm thick highly motile Ascarid. To recover the worm, endoscope was withdrawn along with the basket and the friendly catch. While the endoscope was being withdrawn and the basket was in the duodenum with the worm out of bile duct, patient indicated of relief of abdominal pain. A relook cholangiogram showed no more structures in the duct. She was given antihelmintic therapy and passed hundreds of worms with the feces. The worms recovered form stools were both male and female population and varied in length and size. However the lone worm recovered form bile ducts was the longest and the thickest male worm. The phenomenal behavior of this ubiquitous infection remains unexplained. (Source Records from Dr. Khuroo's Medical Clinic. Review prepared by Mehnaaz Sultan Khuroo Host website www.drkhuroo.org , E-mail: mkhuroo@yahoo.com ).

Simple Continuous Pattern Suture

Male and female Foley catheter insertion into bladder. Using mannequins.
Purpose: To evaluate the results of LASIK and IntraLASIK treatment in myopic patients with nystagmus. Methods: Eight patients with congenital nystagmus (16 eyes), from 23 to 49 years of age, underwent LASIK surgery. Corneal flaps were created using either the Hansatome microkeratome or the Intral...ase femtosecond laser. The ablations were performed with the Bausch & Lomb excimer laser with an active tracking system. In some patients, the eyes were fixated with forceps or a fixation ring during the laser ablation. Results: The refractive errors were corrected in all cases. There was no decentration or loss of best corrected visual acuity greater than 1 line. In 56% of the eyes, the post-operative uncorrected visual acuity was better than the best spectacle corrected-visual acuity (BSCVA). 62.5% of the eyes improved their BSCVA. The overall visual performance was improved in all the patients. One patient that did not not drive before become eligible to get a driver license after the surgery. Conclusions: Selected patients with myopia and congenital nystagmus may benefit from laser refractive surgery. Laser refractive surgery may be safely and accurately performed by using either the Hansatome microkeratome or the Intralase femtosecond laser and an active tracking system with or without mechanical fixation. Certain patients improve their BSCVA post-operatively.

White Fillings

This animated video reviews cochlear implants, used for people with profound hearing loss.

Brachytherapy or localized radiation treatment can be used in certain patients with breast cancer. Depending on tumor size and other factor, physicians may use APBI or accelerated partial breast irradiation. Dr. Elizabeth Tapen, a radiation oncologist, reviews brachytherapy for breast cancer.

Choking Infant Video Demonstration
