- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
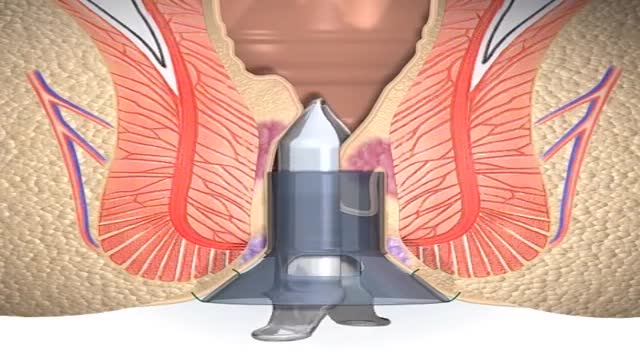
A stapled haemorrhoidopexy is an operation to return the haemorrhoids to a normal. position inside the rectum (back passage). A circular shaped stapling device is gently. inserted in the back passage. The surgeon is then able to use the device to remove.
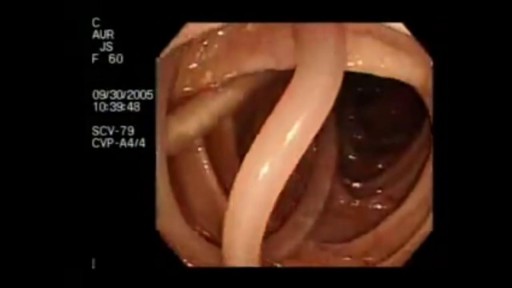
Parasites Accidentally Seen During Colonoscopy

Most of the time, treatment for hemorrhoids involves steps that you can take on your own, such as lifestyle modifications. But sometimes medications or surgical procedures are necessary. Medications If your hemorrhoids produce only mild discomfort, your doctor may suggest over-the-counter creams, ointments, suppositories or pads. These products contain ingredients, such as witch hazel or hydrocortisone, that can relieve pain and itching, at least temporarily. Don't use an over-the-counter cream or other product for more than a week unless directed by your doctor. These products can cause side effects, such as skin rash, inflammation and skin thinning. Minimally invasive procedures If a blood clot has formed within an external hemorrhoid, your doctor can remove the clot with a simple incision, which may provide prompt relief. For persistent bleeding or painful hemorrhoids, your doctor may recommend another minimally invasive procedure. These treatments can be done in your doctor's office or other outpatient setting. Rubber band ligation. Your doctor places one or two tiny rubber bands around the base of an internal hemorrhoid to cut off its circulation. The hemorrhoid withers and falls off within a week. This procedure — called rubber band ligation — is effective for many people. Hemorrhoid banding can be uncomfortable and may cause bleeding, which might begin two to four days after the procedure but is rarely severe. Injection (sclerotherapy). In this procedure, your doctor injects a chemical solution into the hemorrhoid tissue to shrink it. While the injection causes little or no pain, it may be less effective than rubber band ligation. Coagulation (infrared, laser or bipolar). Coagulation techniques use laser or infrared light or heat. They cause small, bleeding, internal hemorrhoids to harden and shrivel. While coagulation has few side effects, it's associated with a higher rate of hemorrhoids coming back (recurrence) than is the rubber band treatment. Surgical procedures If other procedures haven't been successful or you have large hemorrhoids, your doctor may recommend a surgical procedure. Surgery can be performed on an outpatient basis or you may need to stay in the hospital overnight. Hemorrhoid removal. During a hemorrhoidectomy, your surgeon removes excessive tissue that causes bleeding. Various techniques may be used. The surgery may be done with a local anesthetic combined with sedation, a spinal anesthetic or a general anesthetic. Hemorrhoidectomy is the most effective and complete way to treat severe or recurring hemorrhoids. Complications may include temporary difficulty emptying your bladder and urinary tract infections associated with this problem. Most people experience some pain after the procedure. Medications can relieve your pain. Soaking in a warm bath also may help. Hemorrhoid stapling. This procedure, called stapled hemorrhoidectomy or stapled hemorrhoidopexy, blocks blood flow to hemorrhoidal tissue. Stapling generally involves less pain than hemorrhoidectomy and allows an earlier return to regular activities. Compared with hemorrhoidectomy, however, stapling has been associated with a greater risk of recurrence and rectal prolapse, in which part of the rectum protrudes from the anus. Talk with your doctor about what might be the best option for you.
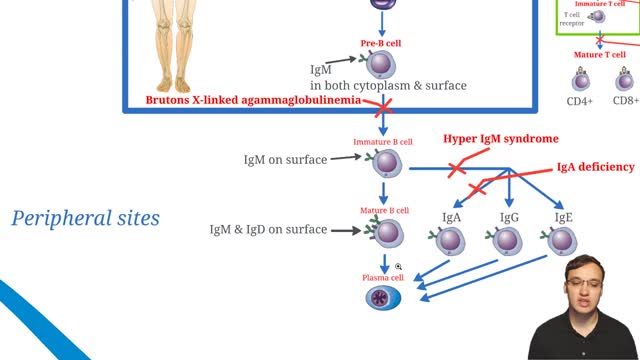
X-linked agammaglobulinemia (XLA), or Bruton agammaglobulinemia, is an inherited immunodeficiency disease caused by mutations in the gene coding for Bruton tyrosine kinase (BTK). The disease was first elucidated by Bruton in 1952, for whom the gene is named. BTK is critical to the maturation of pre–B cells to differentiating mature B cells. The BTK gene defect has been mapped to the long arm of the X chromosome at band Xq21.3 to Xq22, spanning 37.5kb with 19 exons forming 659 amino acids to complete the BTK cytosolic tyrosine kinase. A database of BTK mutations (BTKbase: Mutation registry for X-linked agammaglobulinemia) lists 544 mutation entries from 471 unrelated families showing 341 unique molecular events. No single mutation accounts for more than 3% of mutations in patients. In addition to mutations, a number of variants or polymorphisms have been found.

Frostbite is an injury caused by freezing of the skin and underlying tissues. First your skin becomes very cold and red, then numb, hard and pale. Frostbite is most common on the fingers, toes, nose, ears, cheeks and chin. Exposed skin in cold, windy weather is most vulnerable to frostbite. But frostbite can occur on skin covered by gloves or other clothing.

Drainage of Pus from a Dental Abscess

Dense Hair transplantation with Micro FUE and the Implanter Pen


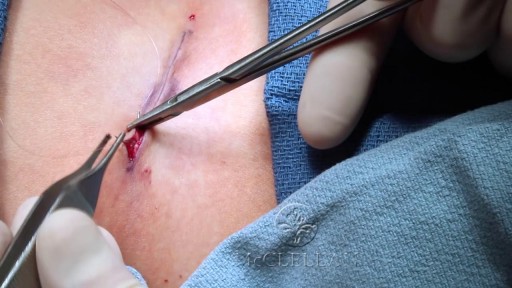
Removal of Infected Hernia Mesh
As the liver becomes more severely damaged, more obvious and serious symptoms can develop, such as: yellowing of the skin and whites of the eyes (jaundice) swelling in the legs, ankles and feet, due to a build-up of fluid (oedema) swelling in your abdomen, due to a build-up of fluid known as ascites.

Gastroschisis is a birth defect that develops in a baby while a woman is pregnant. This condition occurs when an opening forms in the baby's abdominal wall. The baby's bowel pushes through this hole. It then develops outside of the baby's body in the amniotic fluid.
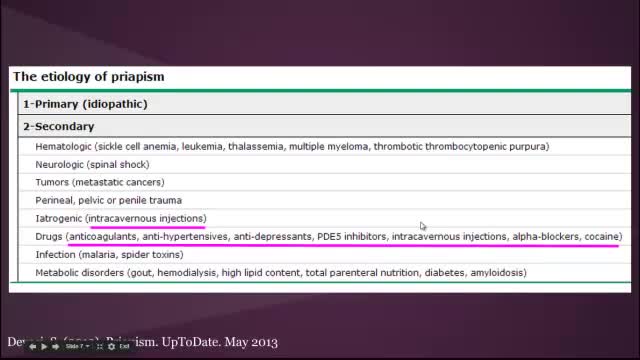
Priapism is a prolonged erection of the penis. The persistent erection continues hours beyond or isn't caused by sexual stimulation. Priapism is usually painful. Although priapism is an uncommon condition overall, it occurs commonly in certain groups, such as people who have sickle cell anemia. Prompt treatment for priapism is usually needed to prevent tissue damage that could result in the inability to get or maintain an erection (erectile dysfunction). Priapism is most common in men in their 30s.
Intussusception (in-tuh-suh-SEP-shun) is a serious condition in which part of the intestine slides into an adjacent part of the intestine. This "telescoping" often blocks food or fluid from passing through. Intussusception also cuts off the blood supply to the part of the intestine that's affected, which can lead to a tear in the bowel (perforation), infection and death of bowel tissue.
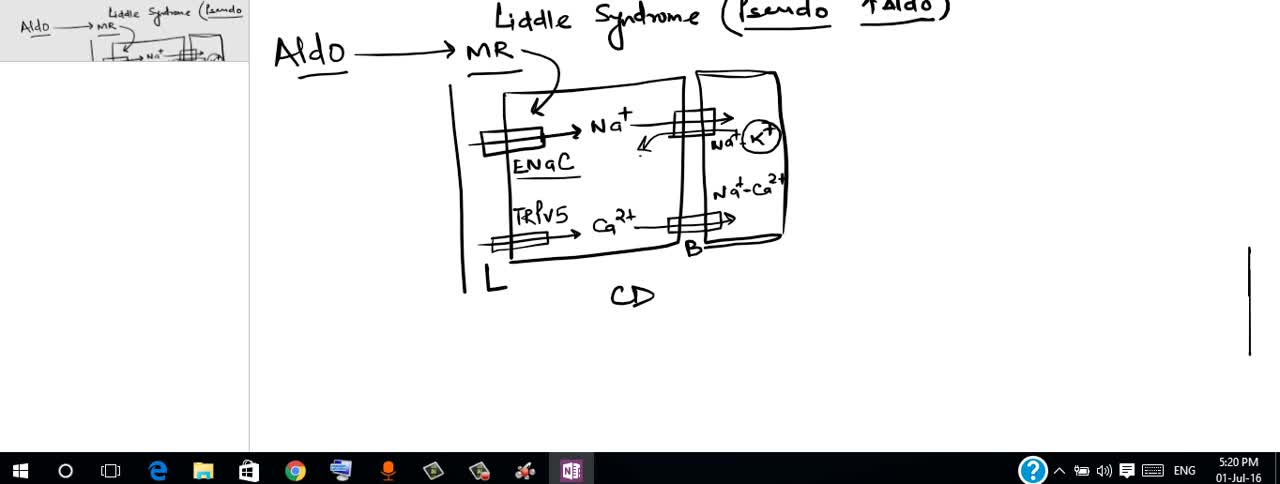
Liddle syndrome is an inherited form of high blood pressure (hypertension). This condition is characterized by severe hypertension that begins unusually early in life, often in childhood, although some affected individuals are not diagnosed until adulthood. Some people with Liddle syndrome have no additional signs or symptoms, especially in childhood. Over time, however, untreated hypertension can lead to heart disease or stroke, which may be fatal.

Parasitic Worm removed from Man's EYE

At URBN Dental, we provide you with top oral hygiene tips to help keep your mouth clean, healthy, and happy. Your manual toothbrush usually comes equipped with a tongue cleaner on the back of its head. That can be helpful in scrubbing your tongue, or you can also use a tongue cleaner. By using simple forward motions on the tongue, you can rid the area of plaque and bacteria which often cause bad breath, gingivitis, and harmful mouth ulcers.
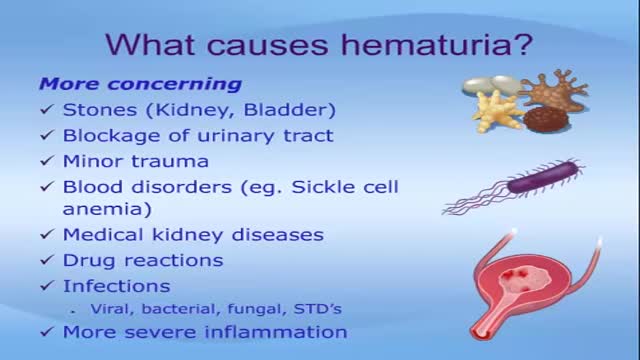
Seeing blood in your urine can cause anxiety. While in many instances there are benign causes, blood in urine (hematuria) can also indicate a serious disorder. Blood that you can see is called gross hematuria. Urinary blood that's visible only under a microscope is known as microscopic hematuria and is found when your doctor tests your urine. Either way, it's important to determine the reason for the bleeding. Treatment depends on the underlying cause.

What Really Happens When You Swallow Gum?
