- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Spina bifida is a condition that affects the spine and is usually apparent at birth. It is a type of neural tube defect (NTD). Spina bifida can happen anywhere along the spine if the neural tube does not close all the way. When the neural tube doesn’t close all the way, the backbone that protects the spinal cord doesn’t form and close as it should. This often results in damage to the spinal cord and nerves. Spina bifida might cause physical and intellectual disabilities that range from mild to severe. The severity depends on: The size and location of the opening in the spine. Whether part of the spinal cord and nerves are affected.

a video showing the technique of Shave and Punch Skin Biopsies nique of
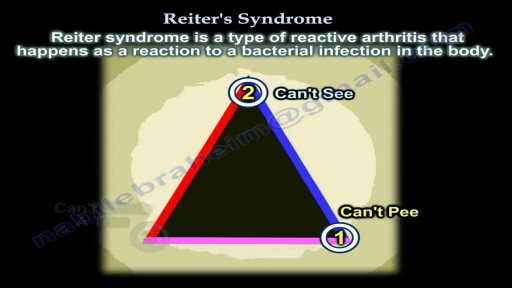
Reiter syndrome is a type of reactive arthritis that happens as a reaction to a bacterial infection in the body. The infection usually happens in the intestines, genitals, or urinary tract. Reiter syndrome includes redness, joint swelling and pain, often in knees, ankles, and feet, along with inflammation of the eyes and urinary tract. It is not contagious. But the bacteria that trigger it can be passed from one person to another. There is no cure for Reiter syndrome, but you can control the symptoms. For most people, symptoms go away in 2 to 6 months.

Keratoderma Blennorrhagicum is a manifestation on the skin that appears in patients diagnosed with reactive arthritis (this condition was previously known as Reiter syndrome). The condition manifests itself by lesions that appear on the skin, initially on the palm of the hands and soles of the feet. The lesions have the tendency to spread, affecting other parts of the body, such as the scrotum, scalp or trunk. Because of their appearance, the lesions might be easily confused with the ones from psoriasis. Keratoderma blennorrhagicum is one of the symptoms that can be used for the clinical diagnosis of reactive arthritis.

Macrobiopsy of breast lesions is a complicated procedure when performed with vacuum assisted biopsy tools. The Spirotome is a hand-held needle set that doesn't need capital investment, is ready to use and provides tissue samples of high quality in substantial amounts. In this way quantitative molecular biology is possible with one tissue sample. The Coramate is an automated version of this direct and frontal technology.

When both mucosa and stroma are parts of the suspect lesion, a deep biopsy is needed. The Cervicore is designed to harvest samples from the cervix and vagina with minimal collateral injury to the surrounding tissues. The procedure is easy with minimal discomfort to the patient.

Endoscopic picture of turban epiglottis in patient of epiglottitis

If your ear is leaking pus, you may have a hole in your eardrum.Your eardrum is stretched across the inner end of your ear canal. It vibrates when sound waves reach it, so you can hear. A hole in your eardrum can be caused by an ear infection. Fluid builds up behind the eardrum. The pressure of the fluid can tear the eardrum. Some people get a hole in the eardrum for other reasons, like hearing a very loud noise. If this happens, the ear may get infected because germs (bacteria) get through the hole. Ear infections happen to adults and children, but they're more common in children. Some things can make you more likely to get an ear infection with discharge. They include getting lots of colds and coughs, living in overcrowded housing, and eating a poor-quality diet

Breast augmentation usually is performed in subglandular, subfascial, or partial submuscular pockets, including the dual plane. A new pocket has been described and used by the author. Methods: From October 2005 to April 2008, 600 patients underwent bilateral breast augme...
ntation using the new technique. Soft cohesive gel micro-textured round implants (range 200- 500cc) were used. The initial pocket is made in the subglandular plane up to the lower level of the nipple areolar complex. The submuscular plane is reached by splitting the pectoralis major muscle at the level of middle and lower third of sternum. The muscle is split along the direction of its fibers up and laterally to the anterior axillary fold. No pectoralis major is released from costal margin. The implant lies in this plane simultaneously behind and in front of the pectoralis major. Procedure is performed as a day case under general anesthetic with no drains. Results: Postoperative analgesia requirements is reduced because of dissection in natural planes resulting in quick recovery. No muscle contraction associated deformities is seen. All patients had aesthetically natural cleavage, with the nipple at the most projected part of the breast with three-dimensional enhancement. Conclusion: An adequate muscle cover of the prosthesis is achieved by muscle splitting breast augmentation technique and the procedure is used in all breast augmentations procedures

Otto Placik MD. a board certified Chicago Illinois based plastic surgeon presents instructional video on post genital surgery (labia minora reduction aka labiaplasty or labioplasty or clitoral hood reduction) massage exercises for treatment of labum minora psot surgical fibrosis or hypersensitivity. Photos pictures and video of anatomic models are reviewed . Great for patients thinking about or planning labiaplasty or vaginal cosmetic surgery

A very funny video

DRE

Letting children patients play the role of a dentist may be a good way to introduce them to the different types of instruments used in a dental clinic. This in turn may also reduce thier anxiety or fear of the dentist and make them more easy-going and compliant towards dental treatments. Ofcourse instruments should be clean and steril and care should be taken to not give them pointed or sharp objects.

Headaches with eating Ice Cream explained by medicine
The procedure of Suprapubic Cystostomy

Open Inguinal Hernia Repair Surgery - German Narration
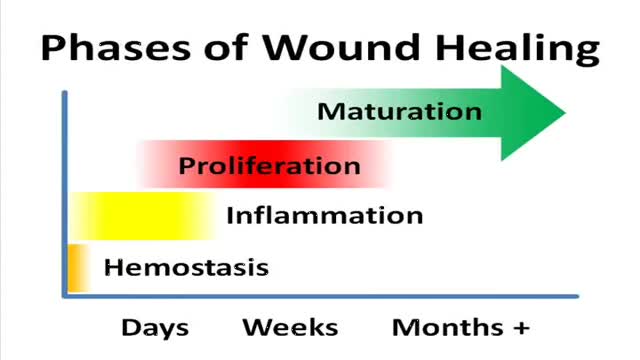
A video showing the phases of normal wound healing

A parasitic twin (also known as an asymmetrical or unequal conjoined twin) is the result of the processes that produce vanishing twins and conjoined twins, and may represent a continuum between the two. Parasitic twins occur when a twin embryo begins developing in utero, but the pair does not fully separate, and one embryo maintains dominant development at the expense of the other. Unlike conjoined twins, one ceases development during gestation and is vestigial to a mostly fully-formed, otherwise healthy individual twin. The undeveloped twin is defined as parasitic, rather than conjoined, because it is incompletely formed or wholly dependent on the body functions of the complete fetus. The independent twin is called the autosite.
Recently a group of affected females from Cameroon has started raising the voices against an old cultural "Female Abuse" tradition which is "Breast Ironing". The point of this tradition is to inhibit the growth of the female breast so that they will avoid getting raped.

Gunshot wounds have become increasing common in urban cities and many such cases can lead to undesirable outcomes. While gunshot wounds to the head are considered most lethal, gunshot wounds to the chest too may be dangerous. Gunshot wound to the chest is challenging owing to the presence of vital organs like lungs, heart and their surrounding structures including major blood vessels. Gunshot wound is caused by penetration of the bullet, which travels through a projectile path after being shot from a firearm. The bullet, on hitting the chest, punctures the tissue it first encounters with, the bones or the muscular chest wall. The extent and severity of the injury depends on the characteristics of the bullet and the firearm, the position and the distance of the victim, the projectile path and the nature of the tissue penetrated.
