- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Ways to Help Pregnant Women Dilate HD
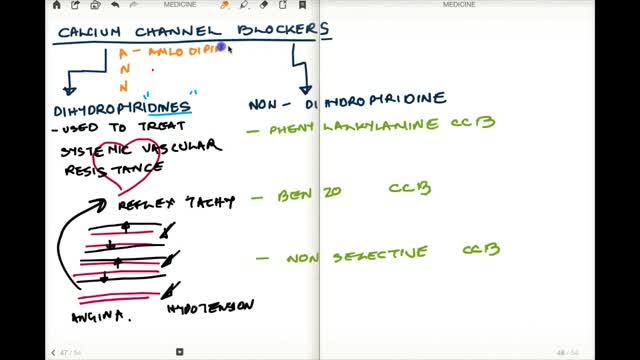
Calcium channel blockers prevent calcium from entering cells of the heart and blood vessel walls, resulting in lower blood pressure. Calcium channel blockers, also called calcium antagonists, relax and widen blood vessels by affecting the muscle cells in the arterial walls. Some calcium channel blockers have the added benefit of slowing your heart rate, which can further reduce blood pressure, relieve chest pain (angina) and control an irregular heartbeat. Examples of calcium channel blockers Some calcium channel blockers are available in short-acting and long-acting forms. Short-acting medications work quickly, but their effects last only a few hours. Long-acting medications are slowly released to provide a longer lasting effect. Several calcium channel blockers are available. Which one is best for you depends on your health and the condition being treated. Examples of calcium channel blockers include: Amlodipine (Norvasc) Diltiazem (Cardizem, Tiazac, others) Felodipine Isradipine Nicardipine Nifedipine (Adalat CC, Afeditab CR, Procardia) Nisoldipine (Sular) Verapamil (Calan, Verelan) In some cases, your doctor might prescribe a calcium channel blocker with other high blood pressure medications or with cholesterol-lowering drugs such as statins.
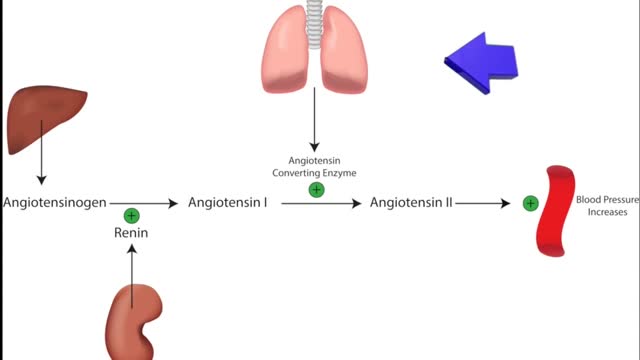
ACE inhibitors Email this page to a friend Print Facebook Twitter Google+ Angiotensin-converting enzyme (ACE) inhibitors are medicines. They treat heart, blood vessel, and kidney problems. How ACE inhibitors help ACE inhibitors are used to treat heart disease. These medicines make your heart work less hard by lowering your blood pressure. This keeps some kinds of heart disease from getting worse. Most people who have heart failure take these medicines. These medicines treat high blood pressure, strokes, or heart attacks. They may help lower your risk for stroke or heart attack. They are also used to treat diabetes and kidney problems. This can help keep your kidneys from getting worse. If you have these problems, ask your health care provider if you should be taking these medicines.
Watch that Above Knee Amputation Surgery video
Digoxin is derived from the leaves of a digitalis plant. Digoxin helps make the heart beat stronger and with a more regular rhythm. Digoxin is also used to treat atrial fibrillation, a heart rhythm disorder of the atria (the upper chambers of the heart that allow blood to flow into the heart).
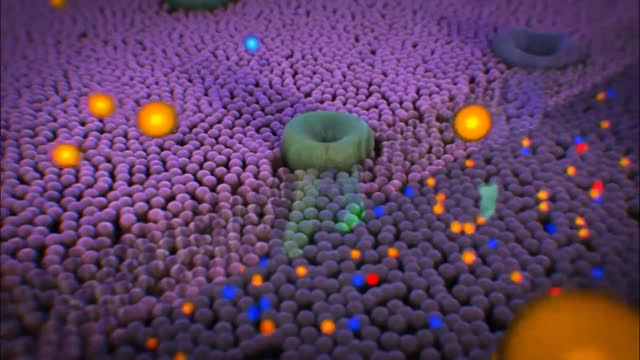
Clopidogrel keeps the platelets in your blood from coagulating (clotting) to prevent unwanted blood clots that can occur with certain heart or blood vessel conditions. Clopidogrel is used to prevent blood clots after a recent heart attack or stroke, and in people with certain disorders of the heart or blood vessels. Clopidogrel may also be used for other purposes not listed in this medication guide

Elbow Exam - Orthopaedic OSCE - Clinical Skills - Dr Gill
The elbow examination is a core skill - in this video, we demonstrate how to perform an elbow EXAM for an Orthopaedic Clinical Skills OSCE, which should be one of the more accessible examination stations for medical students.
For a passing grade in your Clinical Skills OSCE, an elbow assessment should follow the LOOK, FEEL, MOVE approach
Initially looking for erythema, scars, swelling and position
Palpating the elbow - specifically the olecranon, medial and lateral epicondyles, and radial head for heat, oedema and crepitus
Finally assess range of movement with flexion and extension at the elbow, before determining for tennis and golfers' elbows
Watch further orthopaedic examinations for your OSCE revision:
The Elbow - Deep Dive
https://youtu.be/SX5buhtCVDw
The Spine Examination:
https://youtu.be/pJxMHa6SCgU
The Knee examination
https://youtu.be/oyKH4EYfJDM
The Hip examination
https://youtu.be/JC9GKq5nSdQ
The GALS examination
https://youtu.be/5qJaf7gW-B0 - Gait, Arms, Legs, Spine - GALS screen
------------
Please note that there is no ABSOLUTE way to perform a clinical examination. Different institutions and even clinicians will have differing degrees of variations - the aim is the effectively identify medically relevant signs.
However during OSCE assessments. Different medical schools, nursing colleges and other health professional courses will have their own preferred approach to a clinical assessment - you should concentrate on THEIR marks schemes for your assessments.
The examination demonstrated here is derived from Macleods Clinical Examination - a recognised standard textbook for clinical skills.
Some people viewing this medical examination video may experience an ASMR effect
#clinicalskills #Elbow #DrGill

Total Hysterectomy Laparoscopic HD
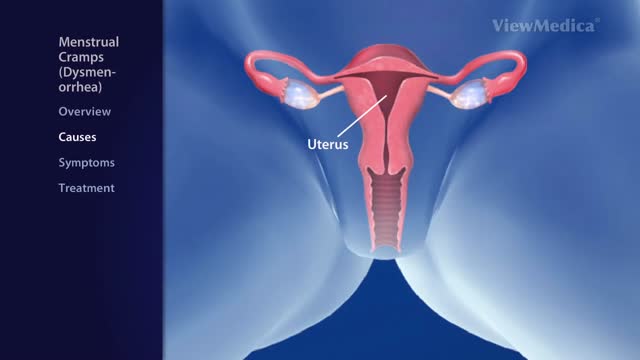
Dysmenorrhea is the medical term for pain with menstruation. There are two types of dysmenorrhea: "primary" and "secondary". Primary dysmenorrhea is common menstrual cramps that are recurrent (come back) and are not due to other diseases. Pain usually begins 1 or 2 days before, or when menstrual bleeding starts, and is felt in the lower abdomen, back, or thighs. Pain can range from mild to severe, can typically last 12 to 72 hours, and can be accompanied by nausea, vomiting, fatigue, and even diarrhea. Common menstrual cramps usually become less painful as a woman ages and may stop entirely if the woman has a baby. Secondary dysmenorrhea is pain that is caused by a disorder in the woman's reproductive organs, such as endometriosis, adenomyosis, uterine fibroids, or infection. Pain from secondary dysmenorrhea usually begins earlier in the menstrual cycle and lasts longer than common menstrual cramps. The pain is not typically accompanied by nausea, vomiting, fatigue, or diarrhea.
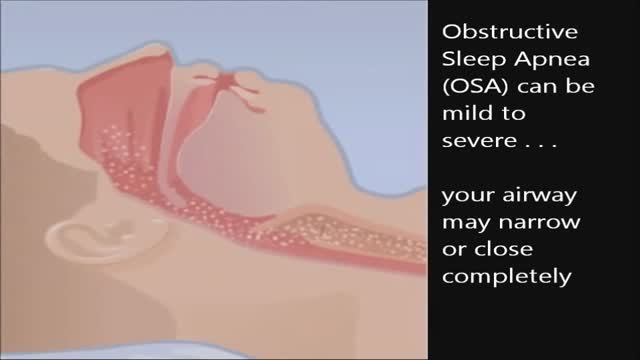
CPAP, or continuous positive airway pressure, is a treatment that uses mild air pressure to keep the airways open. CPAP typically is used by people who have breathing problems, such as sleep apnea. CPAP also may be used to treat preterm infants whose lungs have not fully developed.

Cervical Mucus
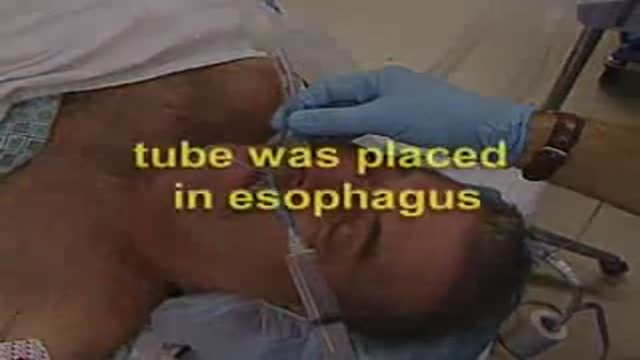
Oesophageal Intubation

Craniopharyngioma Complete Excision
Scientifically Erectile Dysfunction Penile Implants
Menopause is defined as occurring 12 months after your last menstrual period and marks the end of menstrual cycles. Menopause can happen in your 40s or 50s, but the average age is 51 in the United States. Menopause is a natural biological process. Although it also ends fertility, you can stay healthy, vital and sexual. Some women feel relieved because they no longer need to worry about pregnancy. Even so, the physical symptoms, such as hot flashes, and emotional symptoms of menopause may disrupt your sleep, lower your energy or — for some women — trigger anxiety or feelings of sadness and loss. Don't hesitate to seek treatment for symptoms that bother you. Many effective treatments are available, from lifestyle adjustments to hormone therapy.
A stress ulcer is a single or multiple mucosal defect which can become complicated by upper gastrointestinal bleeding during the physiologic stress of serious illness.

Ligation of Aneurysm in ArterioVenous Malformation

Eye Lid Partial Tarsectomy Surgery
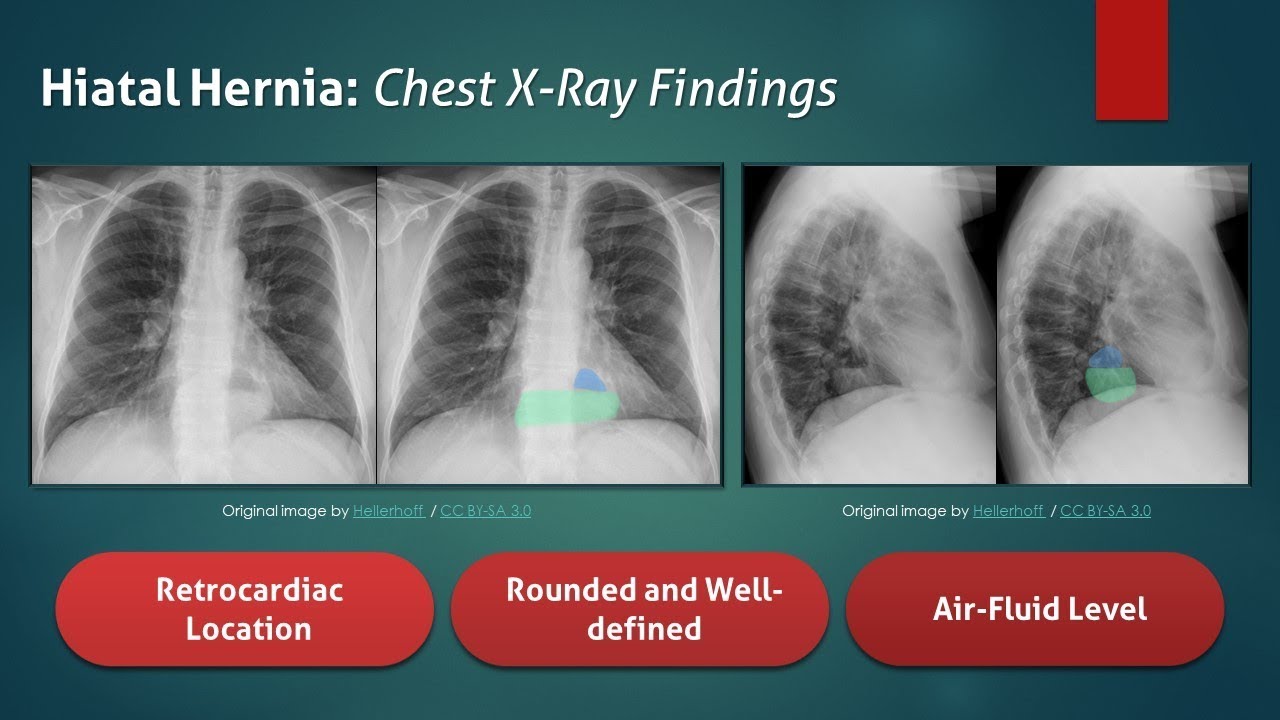
The typical radiograph is of a well-defined, rounded, retrocardiac opacity with an air-fluid level. In this image, the radiolucent gas is highlighted in blue, while the gastric contents are highlighted in the green. In many cases of hiatal hernia, there will not be an air bubble below the left hemidiaphragm. This is a relatively expected finding considering that the stomach is no longer in its usual position. The anatomical position of the herniated organ can be further elucidated on the lateral radiograph. Here we can see that the stomach is in the middle mediastinum posterior to the heart and above the diaphragm. Hiatal hernias can look similar to a retrocardiac lung abscess or another cavitary lesion, but it will change in size and shape between radiographs. Large hernias can shift the mediastinum to the right and result in a widening of the carinal angle. They can even give the appearance of cardiomegaly. In this radiograph, the cardiac silhouette is distinctly visible within the confines of the hiatal hernia. To review, a hiatal hernia on an AP chest radiograph typically appears as a round retrocardiac opacity with an air-fluid level.
🌐 Check out our website for more video lectures
https://www.med4vl.com
📺 Subscribe To My Channel and Get More Great Quizzes and Tutorials
https://www.youtube.com/channe....l/UC95TzSH1B_2EjaZMg
#FOAMrad #MedEd #radiology
Disclaimer: All the information provided by Medical Education for Visual Learners and associated videos are strictly for informational purposes only. It is not intended as a substitute for medical advice from your health care provider or physician. It should not be used to overrule the advice of a qualified healthcare provider, nor to provide advice for emergency medical treatment. If you think that you or someone that you know may be suffering from a medical condition, then please consult your physician or seek immediate medical attention.

Watch that video of Nasty Female Genital Infection
