- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Watch that video to know What is Vaginal Discharge and how to Get Rid of it ?

Urinary incontinence isn't a disease, it's a symptom. It can be caused by everyday habits, underlying medical conditions or physical problems. A thorough evaluation by your doctor can help determine what's behind your incontinence. Temporary urinary incontinence Certain drinks, foods and medications can act as diuretics — stimulating your bladder and increasing your volume of urine. They include: Alcohol Caffeine Decaffeinated tea and coffee Carbonated drinks Artificial sweeteners Corn syrup Foods that are high in spice, sugar or acid, especially citrus fruits Heart and blood pressure medications, sedatives, and muscle relaxants Large doses of vitamins B or C Urinary incontinence also may be caused by an easily treatable medical condition, such as: Urinary tract infection. Infections can irritate your bladder, causing you to have strong urges to urinate, and sometimes incontinence. Other signs and symptoms of urinary tract infection include a burning sensation when you urinate and foul-smelling urine. Constipation. The rectum is located near the bladder and shares many of the same nerves. Hard, compacted stool in your rectum causes these nerves to be overactive and increase urinary frequency. Persistent urinary incontinence Urinary incontinence can also be a persistent condition caused by underlying physical problems or changes, including: Pregnancy. Hormonal changes and the increased weight of the uterus can lead to stress incontinence. Childbirth. Vaginal delivery can weaken muscles needed for bladder control and also damage bladder nerves and supportive tissue, leading to a dropped (prolapsed) pelvic floor. With prolapse, the bladder, uterus, rectum or small intestine can get pushed down from the usual position and protrude into the vagina. Such protrusions can be associated with incontinence. Changes with age. Aging of the bladder muscle can decrease the bladder's capacity to store urine. Menopause. After menopause women produce less estrogen, a hormone that helps keep the lining of the bladder and urethra healthy. Deterioration of these tissues can aggravate incontinence. Hysterectomy. In women, the bladder and uterus are supported by many of the same muscles and ligaments. Any surgery that involves a woman's reproductive system, including removal of the uterus, may damage the supporting pelvic floor muscles, which can lead to incontinence. Enlarged prostate. Especially in older men, incontinence often stems from enlargement of the prostate gland, a condition known as benign prostatic hyperplasia. Prostate cancer. In men, stress incontinence or urge incontinence can be associated with untreated prostate cancer. But more often, incontinence is a side effect of treatments for prostate cancer. Obstruction. A tumor anywhere along your urinary tract can block the normal flow of urine, leading to overflow incontinence. Urinary stones — hard, stone-like masses that form in the bladder — sometimes cause urine leakage. Neurological disorders. Multiple sclerosis, Parkinson's disease, stroke, a brain tumor or a spinal injury can interfere with nerve signals involved in bladder control, causing urinary incontinence.

Tears Of Abortion - Story of an aborted baby,

A VCUG (Voiding Cystourethrogram) is a test that looks at how well your child's kidneys, ureters and bladder are working. Your child's kidneys make urine. The urine flows from the kidneys through thin tubes (called ureters) into your child's bladder.

Foley Catheter Insertion

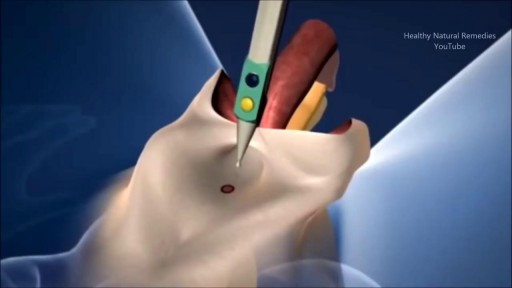
A brain surgery called a craniectomy is performed to remove a part of your skull in order to relieve pressure in an area when your brain swells from a traumatic brain injury. It is also performed to treat medical conditions that cause your brain to swell or bleed that can be caused by an aneurysm, brain tumor or other cancer.
This 3d animation shows how the surgical procedure decreases intracranial pressure (ICP), intracranial hypertension (ICHT), or heavy bleeding (also called hemorrhaging) inside your skull. If left untreated, pressure or bleeding can compress your brain and push it down onto the brain stem. This can be fatal or cause permanent brain damage.
Brain surgery is a very serious procedure under any circumstances, but a craniectomy is done when there is an immediate risk to the brain and neurological function due to severe brain injury or stroke.
For more information about custom 3D animation depicting surgery, please visit https://www.amerra.com/.
Watch additional medical animations:
Accessing an implantable port training - 3D animation: https://youtu.be/xSTpxjyv4O4
Open Suctioning with a Tracheostomy Tube - 3D animation: https://youtu.be/wamB7jpWCiQ
Ventriculostomy Brain Surgery - 3d animation: https://youtu.be/pUy0YDzVNzs
Suctioning the endotracheal tube - medical animation: https://youtu.be/pN6-EYoeh3g
Functional endoscopic sinus surgery (FESS) - 3D animation: https://youtu.be/qKTRyowwaLA
How to insert a nasogastric tube for NG intubation - 3d animation: https://youtu.be/Abf3Gd6AaZQ
Oral airway insertion - oropharyngeal airway technique - 3D animation: https://youtu.be/caxUdNwjt34
Nasotracheal suctioning (NTS) - 3D animation: https://youtu.be/979jWMsF62c
Learn about hemorrhoids with #3d #animation: https://youtu.be/R6NqlMpsiiY
LASIK eye surgery - 3D animation: https://youtu.be/Bb8bnjnEM00
CPR cardiopulmonary resuscitation - 3D animation: https://youtu.be/G87knTZnhks
What are warts (HPV)? - 3D animation: https://youtu.be/guJ1J7rRs1w
How Macular Degeneration Affects Your Vision - 3D animation: https://youtu.be/ozZQIZ_52YY
NeoGraft hair transplant procedure – animation: https://youtu.be/C-eTdH2UPXI
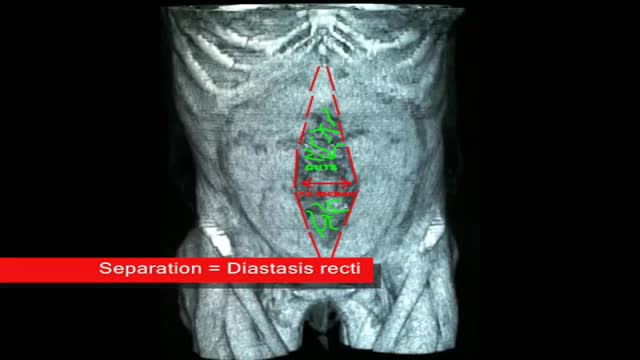
plastic surgeon demonstrates the results of a muscle separation(rectus diastasis) repair using 3 dimesional CAT scan and photographic images
all you need to know about the female orgasm

Dr. Alex Campbell and Dr. Carolina Restrepo of Premium Care Plastic Surgery in Cartagena, Colombia perform a Mommy Makeover on an international patient. Watch the procedure as Dr. Campbell and Dr. Restrepo work together to offer this patient more surgery in less time, which leads to a quicker recovery and better results.
Open heart (coronary artery bypass, or CABG) surgery is performed in order to reroute, or "bypass," blood around blocked arteries, thereby improving the supply of oxygen-rich blood to the heart. Surgeons usually use an artery from the chest wall to construct the "detour" around the blocked part of the artery. Veins from the legs are also used.

The examination room should be quiet, warm and well lit. After you have finished interviewing the patient, provide them with a gown (a.k.a. "Johnny") and leave the room (or draw a separating curtain) while they change. Instruct them to remove all of their clothing (except for briefs) and put on the gown so that the opening is in the rear. Occasionally, patient's will end up using them as ponchos, capes or in other creative ways. While this may make for a more attractive ensemble it will also, unfortunately, interfere with your ability to perform an examination! Prior to measuring vital signs, the patient should have had the opportunity to sit for approximately five minutes so that the values are not affected by the exertion required to walk to the exam room. All measurements are made while the patient is seated. Observation: Before diving in, take a minute or so to look at the patient in their entirety, making your observations, if possible, from an out-of-the way perch. Does the patient seem anxious, in pain, upset? What about their dress and hygiene? Remember, the exam begins as soon as you lay eyes on the patient. Temperature: This is generally obtained using an oral thermometer that provides a digital reading when the sensor is placed under the patient's tongue. As most exam rooms do not have thermometers, it is not necessary to repeat this measurement unless, of course, the recorded value seems discordant with the patient's clinical condition (e.g. they feel hot but reportedly have no fever or vice versa). Depending on the bias of a particular institution, temperature is measured in either Celcius or Farenheit, with a fever defined as greater than 38-38.5 C or 101-101.5 F. Rectal temperatures, which most closely reflect internal or core values, are approximately 1 degree F higher than those obtained orally. Respiratory Rate: Respirations are recorded as breaths per minute. They should be counted for at least 30 seconds as the total number of breaths in a 15 second period is rather small and any miscounting can result in rather large errors when multiplied by 4. Try to do this as surreptitiously as possible so that the patient does not consciously alter their rate of breathing. This can be done by observing the rise and fall of the patient's hospital gown while you appear to be taking their pulse. Normal is between 12 and 20. In general, this measurement offers no relevant information for the routine examination. However, particularly in the setting of cardio-pulmonary illness, it can be a very reliable marker of disease activity. Pulse: This can be measured at any place where there is a large artery (e.g. carotid, femoral, or simply by listening over the heart), though for the sake of convenience it is generally done by palpating the radial impulse. You may find it helpful to feel both radial arteries simultaneously, doubling the sensory input and helping to insure the accuracy of your measurements. Place the tips of your index and middle fingers just proximal to the patients wrist on the thumb side, orienting them so that they are both over the length of the vessel.

Bimanual Hip Examination of the Female genitalia

Dr. Ailawadi, M.D., the Chair of Cardiac Surgery at Michigan Medicine, specializes in minimally invasive valve surgery as well as complex cardiac operations. This video shows step by step footage of a Coronary Artery Bypass Graft (CABG) in a complex patient. In this case, CABG was performed through a sternotomy (through the breast bone) using the internal thoracic artery and saphenous leg veins to bypass obstructed coronary arteries. In this video, Dr. Ailawadi will perform a triple vessel bypass (CABG) which has been shown to minimize the risk of future heart attack and help patients live longer in the setting of complex coronary artery disease.
To learn more about cardiac surgery at Michigan Medicine, visit: https://medicine.umich.edu/dept/cardiac-surgery
To learn more about Frankel Cardiovascular Center, visit: https://www.umcvc.org/
To watch the full playlist, visit: https://www.youtube.com/playli....st?list=PLNxqP-XbH8B
-------------------------------------------------------
Subscribe to Michigan Medicine’s YouTube channel for upcoming videos and future live streams featuring our experts answering your questions.
-------------------------------------------------------
Follow Michigan Medicine on Social:
Twitter: https://twitter.com/umichmedicine
Instagram: https://www.instagram.com/umichmedicine/
Facebook: https://www.facebook.com/MichiganMedicine/
Follow the U-M Frankel Cardiovascular Center on Social:
Twitter: https://twitter.com/umichcvc
Facebook: https://www.facebook.com/Unive....rsityofMichiganCardi
#MichiganMedicine #MedEd #CardiacSurgery #UniversityOfMichiganHealth #FrankelCardiovascularCenter #Cardiology #CardiacSurgeon

Watch this clinical examination video to learn how to diagnose inguinal related groin pain.
This video clip is part of the FIFA Diploma in Football Medicine and the FIFA Medical Network. To enrol or to find our more click on the following link http://www.fifamedicalnetwork.com
The Diploma is a free online course designed to help clinicians learn how to diagnose and manage common football-related injuries and illnesses. There are a total of 42 modules created by football medicine experts. Visit a single page, complete individual modules or finish the entire course.
The network provides the opportunity for clinicians around the world to meet and share ideas relating to football medicine. Ask about an interesting case, debate current practice and discuss treatment strategies. Create a profile and log on to interact with other health professionals from around the globe.
This is not medical advice. The content is intended as educational content for health care professionals and students. If you are a patient, seek care of a health care professional.
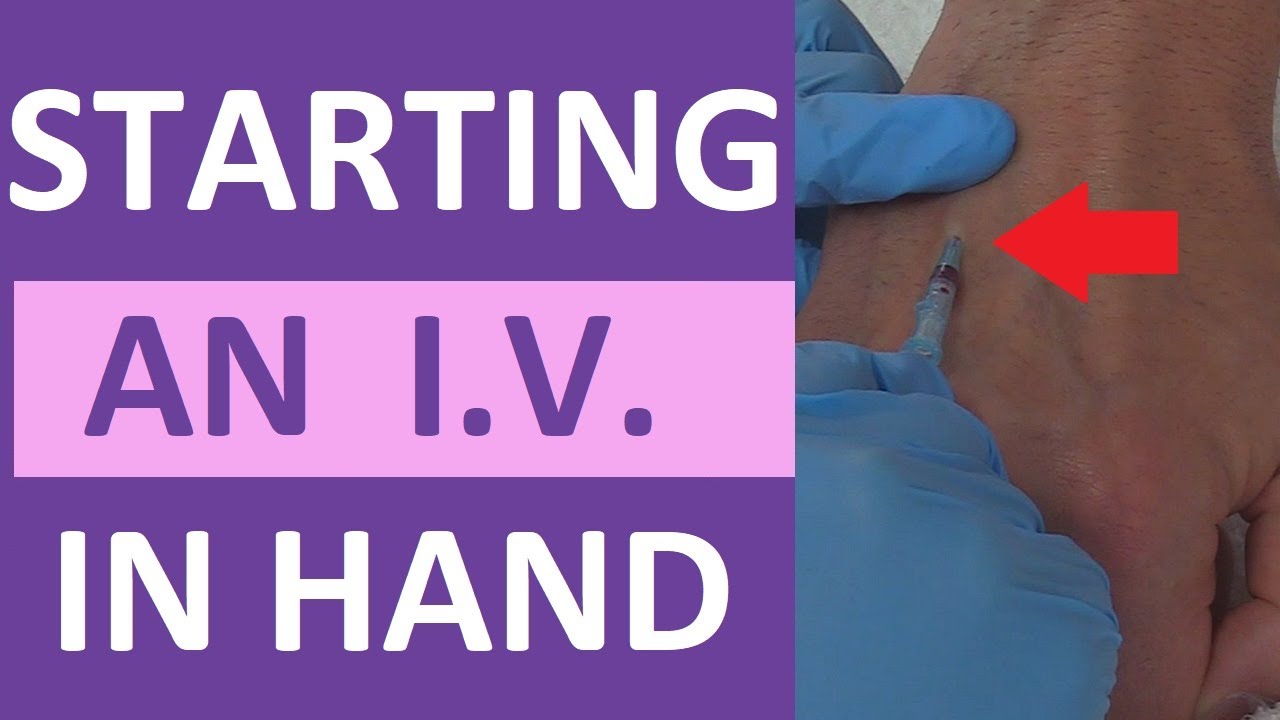
How to start a peripheral IV in the dorsum of the hand: clinical nursing skill technique.
Starting an IV (intravenous catheter) can be an intimidating experience for nurses, especially nursing students and new nurses. However, nurses will perform IV insertions often, so this is an important nursing skill to learn.
Before starting an IV, always follow the protocols of your facility, as well as manufacturer's instructions for any supplies used.
In this video, Nurse Sarah demonstrates how to start a peripheral IV in the dorsum of the hand. Prior to inserting the IV, you'll want to do the following:
-Gather supplies
-Perform hand hygiene
-Prepare supplies (including priming the saline flush, removing air from extension tubing, opening packages, completing labels, and any other steps required by your facility.
-Locate a suitable vein
-Perform hand hygiene
-Don gloves
If the patient has a lot of hair, you might want to use clippers to trim the hairs prior to starting the IV. You may also apply a tourniquet to help veins move near the surface of the skin.
Next, you'll want to clean the site using the cleaner that came in the IV start kit, such as ChloraPrep.
Once the site has dried completely, you can insert the IV. Stabilize the vein with your non-dominant hand, and insert the IV's needle into the vein, watching carefully for blood return (or a blood flash) in the chamber. Advance the IV around 2mm more to ensure the plastic cannula is in the vein, then thread the cannula into the vein and press the needle safety button.
Notes: https://www.registerednursern.....com/how-to-start-an-
IV Video Series: https://www.youtube.com/watch?v=MbG_1-_mnoo&list=PLQrdx7rRsKfXr6kruqEpIovf66sxo0gxh
This video also demonstrates how to flush the IV using the push-pause method, how to secure the IV using the Tegaderm dressing that came with the IV start kit, considerations of the different cap types and the clamp sequence, and more.
For more information, watch the complete tutorial.
#nurse #nursing #iv #startiv #ivtherapy
Website: https://www.registerednursern.com/
More Videos: https://www.youtube.com/watch?v=R2XMro13dD0&list=UUPyMN8DzkFl2__xnTEiGZ1w
Nursing Gear: https://teespring.com/stores/registerednursern
Instagram: https://www.instagram.com/registerednursern_com/
Facebook: https://www.facebook.com/RegisteredNurseRNs
Twitter: https://twitter.com/NursesRN
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf

Amniotomy is the official term for artificially breaking the bag of waters during labor. It is believed that breaking the bag of waters will help to speed up an otherwise slow labor. Amniotomy is part of the Active Management of Labor practiced in some hospitals. Amniotomy is performed by a midwife or doctor. A long, thin instrument with a hook on the end is inserted into the vagina and through the cervix so it can catch and rip the bag of waters. To perform an amniotomy, the cervix must be dilated enough to allow the instrument through the cervix, generally at least a two. Why choose Amniotomy? Unlike other medical methods of starting labor, amniotomy does not add synthetic hormones to your labor. Instead it seems to stimulate your body’s own labor process. Amniotomy allows the use of an internal electronic fetal monitor. How effective is Amniotomy? Amniotomy alone is unpredictable, it may take hours for labor to start with amniotomy. Because amniotomy increases the risk for infection, most caregivers use amniotomy in combination with synthetic oxytocin. Birth does happen faster when amniotomy is combined with synthetic oxytocin than when amniotomy is used alone. Risks of Amniotomy Risks for Mother Increases the risk for infection. This risk is increased with length of time the waters are broken and with vaginal exams. Because of the infection risk, a time limit is given by which the mother must give birth. As the time limit approaches attempts to progress labor will become more aggressive. The fore waters equalize pressure on the cervix so it will open uniformly. When they are broken, the mother increases her chances of having uneven dilation. Risks for Baby Increases the risk of umbilical cord compression. The fore waters equalize pressure on the baby’s head as it presses against the cervix. When they are broken, the pressure on the baby’s head may be uneven causing swelling in some parts.
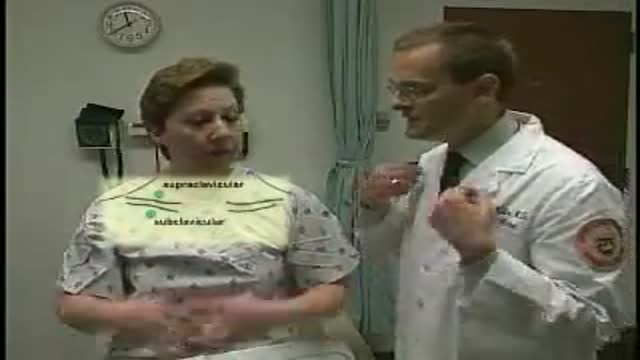
Loyola Breast Examination part 2 Medical breast examination of a female from Loyola University,Chicago
Ever wonder How Male to Female Trans'Gender Surgery works?

Otto Placik MD. a board certified Chicago based plastic surgeon presents Vulvar Vaginal Genital anatomy lesson reviewing the Vulva, Mons Pubis, clitoral hood, prepuce, frenulum, labia minora & majora, vagina, urethra and fourchette with surgical implications and techniques. Photos pictures and video of anatomic models are reviewed in detail on different models. Great for patients thinking about or planning before labiaplasty or vaginal cosmetic surgery
A report of Female Genital Mutilationn FGM (female circucision) in Menya In Egypt تقرير من مدينة المنيا في صعيد مصر عن ختان لاناث
