- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

An abscess is an infectious process characterized by a collection of pus surrounded by inflamed tissue. [1, 2] Abscesses can form anywhere in the body, from a superficial skin (subcutaneous) abscess to deep abscesses in muscle, organs, or body cavities. Patients with subcutaneous skin abscesses present clinically as a firm, localized, painful, erythematous swelling that becomes fluctuant (see the image below).

This animation shows you how a tummy tuck is performed at Boerhaave Medical Centre. Curious? Watch the video!
Boerhaave Medical Centre sets itself the goal of providing the highest quality care. Quality not just in terms of treatment, but also in terms of our staff and the before and after care given. By providing thorough information and clear advice in advance, carefully supporting our patients through the procedure and caring for them afterwards, we believe this quality is assured.
Although we are one of the largest clinics in the Netherlands and have built up many years of experience, we continuously strive to improve. After all, the Boerhaave Medical Centre intends to remain a pioneer in the healthcare sector, by working in accordance with the latest medical findings and techniques both now and in the future.
We offer the highest standard of plastic surgery in our cosmetic care department. For 365 days a year, you can also come to us for non-surgical treatments, such as injectables, permanent hair removal and gastric balloons.
We have been awarded the ZKN quality mark and are certified to ISO 9001-2008 for giving advice and carrying out plastic surgery, including after care.
Visit our website for more information: https://www.boerhaave.com/all-....treatments/upperbody
Follow us:
Facebook: https://www.facebook.com/boerhaavemc
Google+: https://plus.google.com/+BoerhaaveNl-Kliniek
Pinterest: https://nl.pinterest.com/BoerhaaveMC/
Instagram: https://www.instagram.com/BoerhaaveMC/

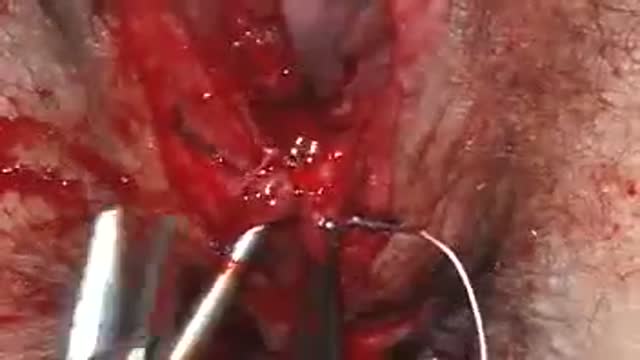
Dr. Debbie Song at Gillette Children's describes in detail selective rhizotomy surgery.
A selective dorsal rhizotomy is an operation performed to treat spasticity. It is thought that high tone and spasticity arise from abnormal signals that are transmitted through sensory or dorsal nerve roots to the spinal cord. In a selective dorsal rhizotomy we identify and cut portions of the dorsal nerve roots that carry abnormal signals thereby disrupting the mechanisms that lead to spasticity. Potential patients go through a rigorous assessment that includes an in-depth gait and motion analysis as well as a physical therapy evaluation.
They are evaluated by a multidisciplinary team that includes a pediatric rehabilitation doctor, a neurosurgeon, and an orthopedist, Appropriate patient selection is vital. Ideal candidates for selective dorsal rhizotomy are children who are between four and ten years of age, have a history of being born prematurely, and have a diagnosis of diplegia cerebral palsy. These patients usually walk independently or with the assistance of crutches or a walker. They typically function at a level one, two, or three in the gross motor function classification system or gmfcs. A selective dorsal rhizotomy involves the coordinated efforts of the neurosurgery, physiatry, anesthesia and nursing teams. The operation entails making an incision in the lower back that is approximately six to eight inches long. We perform what we call a laminoplasty in which we remove the back part of the spinal elements from the lumbar one or l1 to l5 levels. At the end of the procedure the bone is put back on. We identify and open up the Dural sac that contain the spinal fluid spinal cord and nerve roots. Once the Dural sac is opened ,we expose the lumbar and upper sacral nerve roots that transmit information to and from the muscles of the lower extremities.
At each level we isolate the dorsal nerve root, which in turn is separated into as many as 30 smaller thread light fruitlets.
Each rootlet is then electrically stimulated. Specialized members of the physiatry team look for abnormal responses in the muscles of the legs as each rootless is being stimulated. If an abnormal response is observed then the rootlet is cut.
If a normal response is observed, then the rootlet is not cut. We usually end up cutting approximately 20 to 40 percent of the rootlets. The Dural sac is sutured closed and the l1 through l5 spinal elements are put back into anatomic position, thus restoring normal spinal alignment. The overlying tissues and skin are then closed and the patient is awoken from surgery. The entire operation takes between four and five hours. A crucial component to the success of our rhizotomy program is the extensive rehabilitation course following surgery. With their tone significantly reduced after a rhizotomy, patients relearn how to use their muscles to walk more efficiently through stretching, strengthening, and gait training. Approximately one to two years after a rhizotomy patients undergo repeat gait and motion analysis. The orthopedic surgeons assess the need for interventions to correct bone deformities, muscle contractures, poor motor control, impaired balance, or other problems related to cerebral palsy.
At Gillette we work closely with patients and families to ensure that our selective dorsal rhizotomy program meets their goals for enhancing their function and improving their quality of life.
VISIT https://www.gillettechildrens.org/ to learn more
0:00 Why choose selective dorsal rhizotomy?
0:56 Who is a good candidate for selective dorsal rhizotomy?
1:31 What does a selective dorsal rhizotomy entail?
3:26 What is recovery from selective dorsal rhizotomy like?

The most reliable clinical sign to detect ascites is checking for bilateral flank dullness. If a patient with ascites is lying supine, fluid accumulates in the flank regions, leading to dullness on percussion. At the same time, the air-filled bowel loops are forced upwards by the free fluid due to buoyancy, resulting in tympanitic percussion. To locate specifically where dullness shifts to tympany, or the air-fluid level, percussion should be performed from the sides towards the middle. To confirm that the dullness is caused by ascites, ask the patient to switch to a lateral decubitus position. If ascites is present, the air-filled bowel loops will shift accordingly and remain at the surface of the fluid. As a result, the air-fluid level will shift as well. This is known as shifting dullness.
Subscribe to AMBOSS YouTube for the latest clinical examination videos, medical student interviews, study tips and tricks, and live webinars!
Free 5 Day Trial: https://go.amboss.com/amboss-YT
Instagram: https://www.instagram.com/amboss_med/
Facebook: https://www.facebook.com/AMBOSS.Med/
Twitter: https://twitter.com/ambossmed
Blog: https://blog.amboss.com/us
#AMBOSSMed #ClinicalExamination

This video is really sad. You can literally watch this man dying. He was shot in the chest and rushed to the emergency room. His heart has stopped beating or has arrested. As a last resort, surgeons did an extreme procedure called an open thoracotomy which is that crazy tool you see there that basically splits the ribs open and allows easy open access to the heart. They did this so they could give him a cardiac massage. A cardiac massage is when surgeons are manually trying to pump the heart after it has stopped working on its own (cardiac arrest). Unfortunately he lost so much blood from his gun shot wound and he was pronounced dead. There are cases of patients surviving after having this kind of invasive resuscitation but it is rare.

Watch that video to know How to Insert Enema

A vaginoplasty is a surgical procedure that tightens the vagina. This is done by removing excess vaginal lining and tightening the surrounding soft tissues and muscles. During delivery of a baby the vagina and surrounding tissues and muscles become stretched. After delivery the vagina may return to a more “normal” size, but it often fails to return to its’ pre pregnancy diameter. Generally, the more vaginal deliveries, the worse the condition gets. Many women will complain of decreased sensation and sexual satisfaction during intercourse. Commonly this is due to a lack of friction. Often their partner may notice a change although he may say nothing. Kegel exercises are often recommended but rarely succeed in restoring vaginal tightness.

Tummy Tuck ( Classic Method ) : Surgery | 3D Animation
How long does tummy tuck last?
Tummy tuck results are considered permanent, insofar that the fat cells and skin removed during an abdominoplasty cannot grow back. Likewise, the internal sutures placed to repair abdominal muscles are designed to remain in place indefinitely.
What is tummy tuck surgery?
A tummy tuck — also known as abdominoplasty — is a cosmetic surgical procedure to improve the shape and appearance of the abdomen. During a tummy tuck, excess skin and fat are removed from the abdomen. Connective tissue in the abdomen (fascia) usually is tightened with sutures as well.
How much does tummy tuck cost?
How much does it cost? It can cost from about £5,000 to £10,000 to have an abdominoplasty in the UK, plus the cost of any consultations or follow-up care.
How painful is a tummy tuck?
A tummy tuck requires significant downtime
At the beginning, you will be fatigued, swollen and sore. It is normal to have moderate pain during these first several days, although this will steadily improve. It is vital to allow yourself time to focus on rest and healing.
What is the disadvantage of tummy tuck?
The cons of a tummy tuck include: A full abdominoplasty is a major operation with a considerable recovery. Expect to postpone strenuous activities for at least 6 weeks. Results take time.
Is tummy tuck more painful than C section?
That's something many women want to know. While patients have different experiences, most plastic surgeons would agree that a cesarean section is more painful than most tummy tucks.
- Tummy tuck
- Abdominoplasty
- Abdominal tuck
- Tummy tuck procedure
- Tummy tuck process
- Tummy tuck surgery
- Tummy tuck operation
- Tummy tuck video
- Tummy tuck recovery
- Tummy tuck before and after
- Abdominoplasty surgery
- Abdominal contouring surgery
- Postpartum tummy tuck
- Post pregnancy tummy tuck
- Mini tummy tuck
- Tummy tuck cost
- Tummy tuck risks
- Tummy tuck complications
- How long does a tummy tuck take
- Tummy tuck scarring
- Tummy tuck skin removal
- Tummy tuck muscle tightening
#tummytuck
#abdominoplasty
#plastic_surgery
#cosmetic_surgery
#body_contouring
#tummy_tuck_surgery
#surgery
#cosmetic_procedure
#beauty
#health
#fitness
#medical_animation
#3d_animation
#medical_video
#explainer_video
#education

this video shows how the adult circumcision is easy by the alisklamp

Lesson on clinical examination of a scaphoid fracture and assessment of the anatomic snuffbox. The scaphoid bone is one of the carpal bones of the wrist. A scaphoid fracture is important to rule out due to risk of avascular necrosis, which is a compromise of bone vasculature leading to death of the bone. Scaphoid fractures can occur with a FOOSH injury. In this lesson, we discuss the clinical assessment to rule out a scaphoid fracture, including assessing and localizing the anatomic snuffbox.
If you find this lesson helpful, please consider liking, subscribing, and clicking the notification bell to help support this channel and stay up-to-date on future lessons.
*Subscribe for more free medical lessons* https://www.youtube.com/channe....l/UCFPvnkCZbHfBvV8Ap
-------------------------------------------------------------------------------------------------------------
For books and more information on these topics
https://www.amazon.com/shop/jjmedicine
Support future lessons (and get other cool stuff) ➜ https://www.patreon.com/jjmedicine
Follow me on Twitter! ➜ https://twitter.com/JJ_Medicine
Come join me on Facebook! ➜ https://www.facebook.com/JJ-Me....dicine-1006426481611
Start your own website with BlueHost ➜ https://www.bluehost.com/track/jjmedicine/
Check out the best tool to help grow your YouTube channel (it’s helped me!)
https://www.tubebuddy.com/jjmedicine
-------------------------------------------------------------------------------------------------------------
Check out some of my other lessons.
Medical Terminology - The Basics - Lesson 1:
https://www.youtube.com/watch?v=04Wh2E9oNug
Fatty Acid Synthesis Pathway:
https://www.youtube.com/watch?v=WuQS_LpNMzo
Wnt/B Catenin Signaling Pathway:
https://www.youtube.com/watch?v=NGVP4J9jpgs
Upper vs. Lower Motor Neuron Lesions:
https://www.youtube.com/watch?v=itNd74V53ng
Lesson on the Purine Synthesis and Salvage Pathway:
https://www.youtube.com/watch?v=e2KFVvI8Akk
Gastrulation | Formation of Germ Layers:
https://www.youtube.com/watch?v=d6Kkn0SECJ4
Introductory lesson on Autophagy (Macroautophagy):
https://www.youtube.com/watch?v=UmSVKzHc5yA
Infectious Disease Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Dermatology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Pharmacology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Hematology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Rheumatology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Endocrinology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Nephrology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
----------------------------------------------------------------------------------------------------
**MEDICAL DISCLAIMER**: JJ Medicine does not provide medical advice, and the information available on this channel does not offer a diagnosis or advice regarding treatment. Information presented in these lessons is for educational purposes ONLY, and information presented here is not to be used as an alternative to a healthcare professional’s diagnosis and treatment of any person/animal.
Only a physician or other licensed healthcare professional are able to determine the requirement for medical assistance to be given to a patient. Please seek the advice of your physician or other licensed healthcare provider if you have any questions regarding a medical condition.
----------------------------------------------------------------------------------------------------
*Although I try my best to present accurate information, there may be mistakes in this video. If you do see any mistakes with information in this lesson, please comment and let me know.*
I am always looking for ways to improve my lessons! Please don't hesitate to leave me feedback and comments - all of your feedback is greatly appreciated! :) And please don't hesitate to send me any messages if you need any help - I will try my best to be here to help you guys :)
Thanks for watching! If you found this video helpful, please like and subscribe!
JJ
A report of Female Genital Mutilationn FGM (female circucision) in Menya In Egypt تقرير من مدينة المنيا في صعيد مصر عن ختان لاناث

Watch that video to know What is Vaginal Discharge and how to Get Rid of it ?
A video showing the repair of episiotomy
Immune Responses During a Lupus Flare Video

Watch that Full Human Body Decay Process Video

An ectopic pregnancy (EP) is a condition in which a fertilized egg settles and grows in any location other than the inner lining of the uterus. The vast majority of ectopic pregnancies are so-called tubal pregnancies and occur in the Fallopian tube.

Best and 100% Successful Hymen Repair Surgery in Delhi with Latest Ultrafine Hymen repair Technology. 100% successful , Secure and Private. for more information visit: http://www.olmeccosmeticsurgery.com/best-hymenoplasty-surgery-india-delhi/

Tears Of Abortion - Story of an aborted baby,

Female condoms are easy to use with a little practice. Here are the basics on how to insert, use, and remove a female condom.

The products of a surgical abortion.
