- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
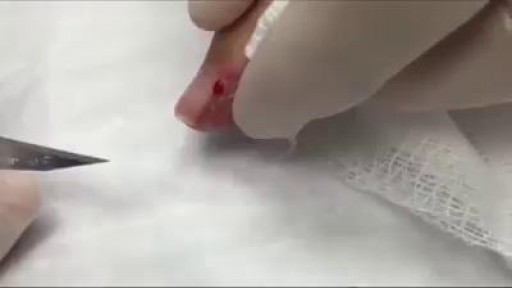
Paronychias are most often caused by common skin bacteria (most commonly staphylococci bacteria) entering the skin around the nail that has been damaged by trauma, such as nail biting, finger sucking, dishwashing, or chemical irritants. Fungal infection also can be a cause of paronychia formation and should be considered especially in people with recurrent infection. Paronychia should not be confused with herpetic whitlow, which can form tiny pustules on the finger and is caused by a virus but is not typically located at the nail edge. Herpetic whitlow is not treated with an incision and drainage and therefore needs to be distinguished from a paronychia.

Rapid cycling is a pattern of frequent, distinct episodes in bipolar disorder. In rapid cycling, a person with the disorder experiences four or more episodes of mania or depression in one year

Gastrostomy tube is placed when a patient is not able to eat on his/her own as a result of neurological or other dysfunction. There are many different types of gastrostomy tubes but in general there are two bigger categories. The classic one and the low profile one. The gastroplexy technique is used preferably to avoid accidental pulling of the gastrostomy tube from an agitated or confused patient.
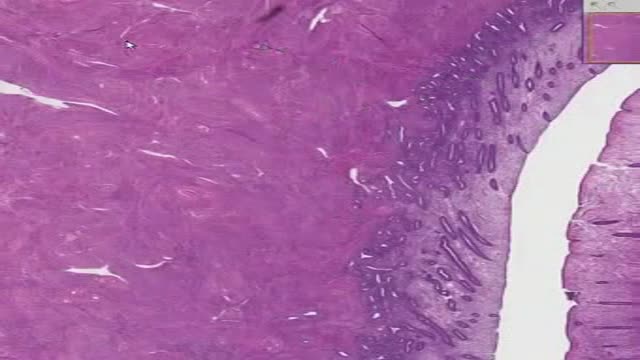
Histology of Dense Bone

DermaClinix, The world's leading hair Transplantation and aesthetic dermatology clinic that offers the best hair transplant in Chennai. The clinic is fully equipped with infrastructure and the ultra-modern devices in the field of cosmetology and hair restoration. At DermaClinx Chennai offers a number of treatments including chemical peels for acne, pigmentation treatment, glow facials, hair growth therapies and many more. Hair transplant Doctors at DermaClinix Nungambakkam, Chennai have more than 12 years of experience in this field & holds the International accreditations and member of ISHRS (USA). Visit us today to know more about the hair growth treatments. https://www.dermatologistchennai.in/hair-transplant-surgeon-in-chennai.php Address: No:19 1st Floor TMA Tower Dr.Thirumurthy Nagar main road, Nungambakkam, Chennai, Tamil Nadu 600034 Call us at - +918939636222, +91 89398 81919 For more: Website - https://www.hairtransplantchennai.org/ Email - enquiry@hairtransplantchennai.org

Most healthy children are inattentive, hyperactive or impulsive at one time or another. It’s normal for preschoolers to have short attention spans and be unable to stick with one activity for long. Even in older children and teenagers, attention span often depends on the level of interest. The same is true of hyperactivity. Young children are naturally energetic — they often are still full of energy long after they’ve worn their parents out. In addition, some children just naturally have a higher activity level than others do. Children should never be classified as having ADHD just because they’re different from their friends or siblings. Children who have problems in school but get along well at home or with friends are likely struggling with something other than ADHD. The same is true of children who are hyperactive or inattentive at home, but whose schoolwork and friendships remain unaffected.
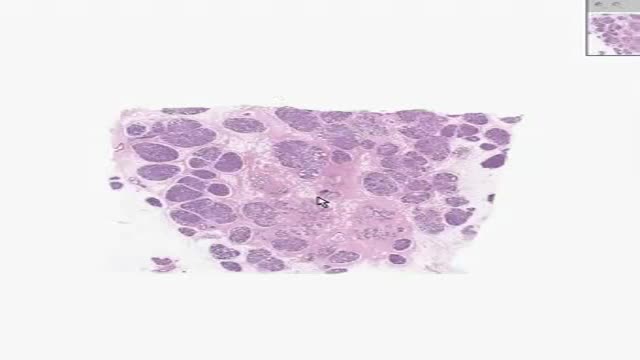
Histology of Active Breast
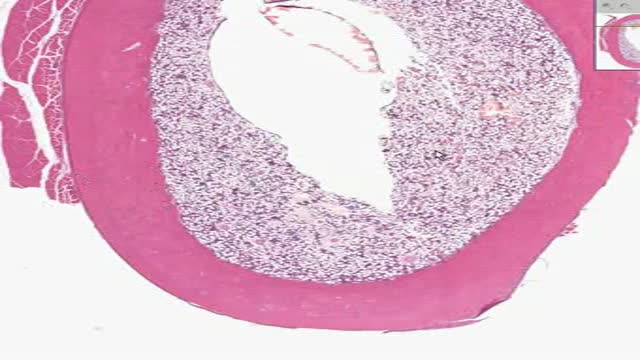
Histology of Uterus

Eyeball cyst Removal
Watch that Huge Nose Booger Removal


Elizabeth Stephens, MD joined the Department of Cardiovascular Surgery at Mayo Clinic Rochester, Minnesota in 2019. To learn more about Dr. Stephens’ practice: https://www.mayoclinic.org/bio....graphies/stephens-el
Elizabeth H. Stephens, M.D., Ph.D., is an Assistant Professor of Surgery in Cardiovascular Surgery specializing in congenital cardiac surgery. She received her medical degree from Baylor College of Medicine and Ph.D in Bioengineering from Rice University focusing on tissue engineering heart valves. Her adult cardiothoracic training was completed at Columbia University and congenital training at Lurie Children's Hospital in Chicago. Her clinical areas of expertise include the treatment of:
• Neonates, infants, and children with complex congenital heart disease
• Adult patients with congenital heart disease, including patients previously repaired
• Valve disease, including Ebstein's anomaly
• Pediatric patients with heart failure, including mechanical circulatory support and heart transplantation
• Patients with vascular rings and tracheal stenosis
In addition to her clinical areas of expertise, Dr. Stephens is active in outcomes research relative to congenital heart disease and is extensively published on various cardiac surgery conditions. She has a particular interest in education, including serving on national committees and mentoring trainees of all levels.
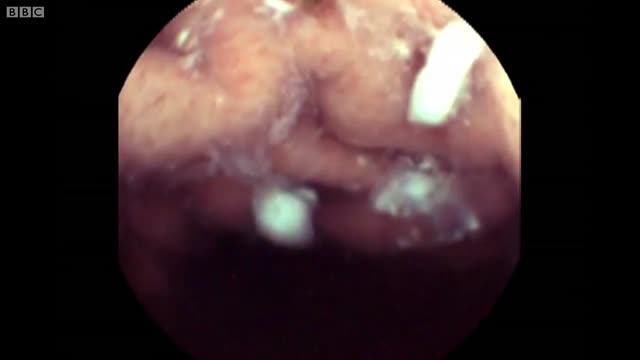
There’s a strange, mysterious world inside us, an alien-looking environment that turns the food we eat into nutrients that keep us alive. Michael Mosley swallows a camera to take a closer look.

A visual prosthesis, often referred to as a bionic eye, is an experimental visual device intended to restore functional vision in those suffering from partial or total blindness. In 1983 Joao Lobo Antunes, a Portuguese doctor, implanted a bionic eye in a person born blind.

Ganglion Cyst Removal
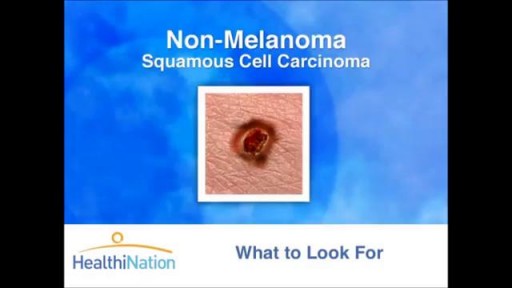
The Skin Cancer Foundation, founded in 1979 by dermatologist and Mohs surgeon Perry Robins, MD, is a global organization solely devoted to educating the public and medical community about skin cancer prevention, early detection, and treatment

Dysmenorrhea, or chronic menstrual pain, is the most common gynecological pain condition, affecting from 45% to 95% of menstruating women. But because it is commonly considered a normal aspect of the menstrual cycle,

From UW Health's Neurosurgery Program: Learn more about the individual steps in the DBS surgery procedure. Visit uwhealth.org/dbs

Psychotic Depression Information

