- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

#abdomenliposuction #laserskintightening #drprashantyadav #cosmeticsurgery #plasticsurgery #dezireclinicindia #weightloss #shorts #360degreeabdomenliposuction #lowerbackliposuction
Weight Loss After 360° Abdomen liposuction result, Abdomen Liposuction, lower back liposuction, 360 degree abdomen liposuction
☎️ For more info:
WhatsApp Your Details to know the Cost
Delhi - 8956880644, 9717470550, Pune - 9222122122, Bangalore- 8971224700, Gurugram - 9272007896, Ahmedabad - 9711162746
Why choose Dezire Clinic For Your Cosmetic and plastic surgery treatment ?
Dezire Clinic is a top searched clinic surgical and nonsurgical cosmetic procedure in India when comes to “Cosmetic, Skin ,Laser and Hair transplantation”.
Like and Share the video if you find it useful. Do not forget to Subscribe to our channel to get more updates.
Subscribe on YouTube https://youtube.com/dezireclin....ic?sub_confirmation=
https://youtube.com/dezireplas....ticsurgerycenter?sub
🎦 https://www.youtube.com/dezireclinic
🎦 https://www.youtube.com/DezirePlasticSurgeryCenter
👍🏻 https://www.facebook.com/drprashantmch/
👍🏻 https://www.facebook.com/dezireclinic
📸 https://www.instagram.com/drprashantdezireclinic/
📸 https://www.instagram.com/dezireclinics/
🐥 https://twitter.com/drprashantmch
👍🏻 https://www.linkedin.com/in/drprashantyadav/
🌐 Website: https://www.dezireclinic.in/
📧 dezireclinicindia@gmail.com
📧 info@dezireclinic.in
Dr. Prashant Yadav (M.S., M.Ch. Plastic Surgery ) & Founder of Dezire Clinic
Disclaimer: The content of this channel is for informational and educational purposes only. This content should not be considered a substitute for advice provided by a certified plastic or cosmetic surgeon. Patients must be properly diagnosed by a healthcare professional on an individual basis in order to achieve the desired results. There is no guarantee of getting the results and outcomes shown in videos, as the results can vary at the end. We will not be held liable for any harm caused by someone misusing our name.
#plasticsurgery #cosmeticsurgery #dezireclinic #drprashantyadav


This condition is seen in imperforate hymen or transverse vaginal septum. Pt presents with primary amenorrhea. Dr Hemant Damle Prof Dept of OBGYN SKNMC Pune India
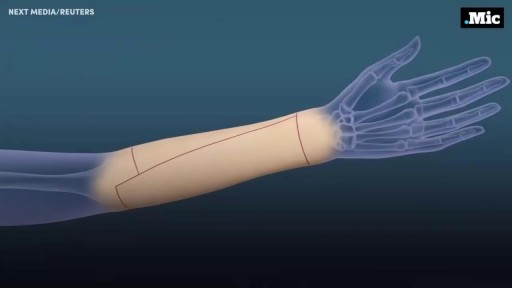
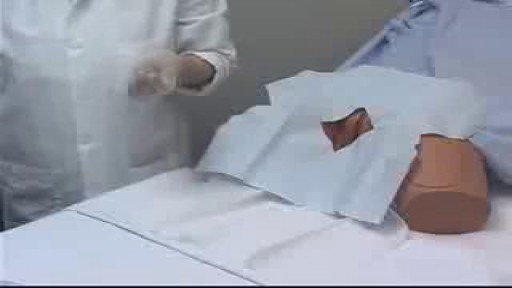
Here's how female-to-male gender reassignment surgery works.

Hand hygiene for healthcare workers: Learn how to perform hand washing with soap and water (nursing procedures).
There are two ways to perform hand hygiene as a nurse. You can use soap and water or an alcohol-based hand rub (also called hand sanitizer or hand gel).
Hand hygiene is essential for providing safe patient care. If hand hygiene is not performed regularly, germs can be easily be spread to patients, other healthcare workers, and even yourself.
Hand hygiene is ALWAYS performed before and after patient care, after coming into contact with any type of body fluid or open wounds, when touching any object that is near a patient (hand railing, bedside table etc.), removing gloves, prior to eating, or after using the bathroom.
This video discusses when you should use soap and water versus an alcohol-based hand gel, when to perform hand hygiene, and demonstrates how to perform hand hygiene using soap and water.
Notes: https://www.registerednursern.....com/how-to-perform-h
More nursing skills: https://www.youtube.com/watch?v=DBHnd3N-5Ns&list=PLQrdx7rRsKfUhd_qQYEbp0Eab3uUKhgKb
Facebook: https://www.facebook.com/RegisteredNurseRNs
Instagram: https://www.instagram.com/registerednursern_com/
Twitter: https://twitter.com/NursesRN
#handhygiene #handwashing #nursingskills
Subscribe: http://www.youtube.com/subscri....ption_center?add_use
Nursing School Supplies: https://www.registerednursern.....com/the-ultimate-lis
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing School Study Tips: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing School Tips & Questions" https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Teaching Tutorials: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Types of Nursing Specialties: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Healthcare Salary Information: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
New Nurse Tips: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Career Help: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
EKG Teaching Tutorials: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Dosage & Calculations for Nurses: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Diabetes Health Managment: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf

Watch that Vaginal Lips Trimming Surgery

External ring Invagination
Internal ring occlusion test
History Inspection Palpation
taxis
Zieman

Female Catheter Insertion
Testicular Self Exam
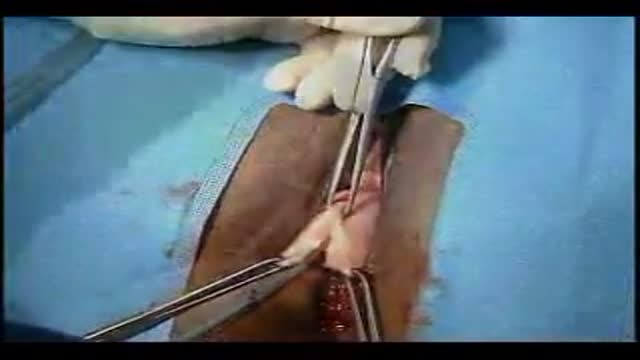
Anterior and Posterior Vaginal Repair Plus IVS Tunne

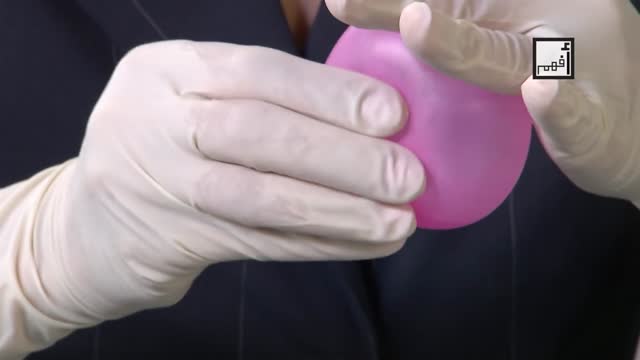
Ganglion cysts are noncancerous lumps that most commonly develop along the tendons or joints of your wrists or hands. They also may occur in the ankles and feet. Ganglion cysts are typically round or oval and are filled with a jellylike fluid. Small ganglion cysts can be pea-sized, while larger ones can be around an inch (2.5 centimeters) in diameter. Ganglion cysts can be painful if they press on a nearby nerve. Their location can sometimes interfere with joint movement. If your ganglion cyst is causing you problems, your doctor may suggest trying to drain the cyst with a needle. Removing the cyst surgically also is an option. But if you have no symptoms, no treatment is necessary. In many cases, the cysts go away on their own.

Health Assessment: Musculoskeletal System- Nursing Skills
FREE Nursing School Cheat Sheets at: http://www.NURSING.com
Get the full lesson on musculoskeletal assessment here:
https://nursing.com/lesson/02-11-musculoskeletal/
Welcome to the NURSING Family, we call it the most supportive nursing cohort on the planet.
At NURSING.com, we want to help you remove the stress and overwhelm of nursing school so that you can focus on becoming an amazing nurse.
Check out our freebies and learn more at: (http://www.nursing.com)
Health Assessment: Musculoskeletal System- Nursing Skills:
In this video we’re going to review a Musculoskeletal Assessment. The Musculoskeletal system involves the muscles, bones, and joints. This means we must assess structure AND function! If the patient cannot stand, assessments should be performed in the bed to the best of your ability. If they cannot perform Active Range of Motion (ROM), use Passive movements to determine ROM.
We love you guys! Go out and be your best selves today! And, as always, happy nursing!
Bookmarks:
0.05 Introduction
0:34 Spine assessment
1:02 Range of motion
1:39 Extremity assessment
1:52 Shoulder range of motion
2:10 Elbow & wrist range of motion
2:25 Hand range of motion
2:34 Upper extremity strength
2:54 Lower extremity range of motion
3:02 Hips range of motion
3:20 Knees range of motion
3:30 Ankles range of motion
3:38 Toes range of motion
3:42 Lower extremity strength
4:05 Outro
Visit us at https://nursing.com/medical-disclaimer/ for disclaimer information.
NCLEX®, NCLEX-RN® are registered trademarks of the National Council of State Boards of Nursing, INC. and hold no affiliation with NURSING.com.

a video of abdominal physical examination including all the required items:
-Inspection
-Palpation
-Percussion
-Auscultation
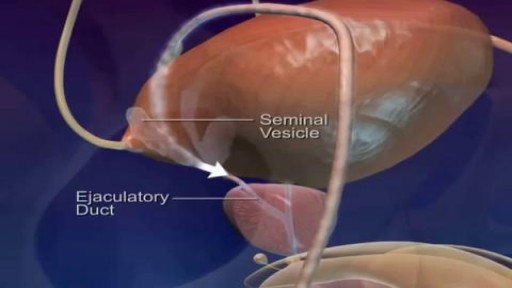
Watch that video of Pathway and Ejaculation of Sperm

How female-to-male gender reassignment surgery works

Endoscopy in Hiatal Hernia.
ACTUAL CATHETERIZATION A clinical view of insertion into the male urethra. A 14 french coude cath was used.
Anatomy of Love

Breast masses are broadly classified as benign or malignant. Common causes of a benign breast mass include fibrocystic disease, fibroadenoma (see the image below), intraductal papilloma, and abscess.
