- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Penile implants are devices placed inside the penis to allow men with erectile dysfunction (ED) to get an erection. Penile implants are typically recommended after other treatments for ED fail. There are two main types of penile implants, semirigid and inflatable.
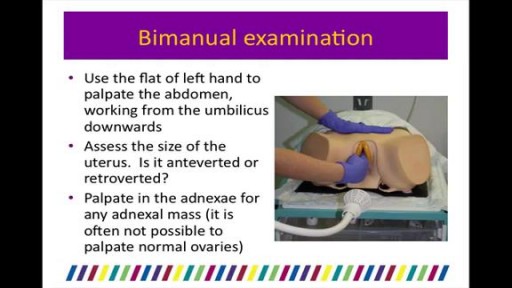
our uterus (or womb) is normally held in place inside your pelvis with various muscles, tissue, and ligaments. Because of pregnancy, childbirth or difficult labor and delivery, in some women these muscles weaken. Also, as a woman ages and with a natural loss of the hormone estrogen, her uterus can drop into the vaginal canal, causing the condition known as a prolapsed uterus.

This video is really sad. You can literally watch this man dying. He was shot in the chest and rushed to the emergency room. His heart has stopped beating or has arrested. As a last resort, surgeons did an extreme procedure called an open thoracotomy which is that crazy tool you see there that basically splits the ribs open and allows easy open access to the heart. They did this so they could give him a cardiac massage. A cardiac massage is when surgeons are manually trying to pump the heart after it has stopped working on its own (cardiac arrest). Unfortunately he lost so much blood from his gun shot wound and he was pronounced dead. There are cases of patients surviving after having this kind of invasive resuscitation but it is rare.

Focal seizures (also called partial seizures [citation needed] and localized seizures) are seizures which affect initially only one hemisphere of the brain. [citation needed] The brain is divided into two hemispheres, each consisting of four lobes – the frontal, temporal, parietal and occipital lobes.
http://www.wss4m.com/vb

The Epley Maneuver for Vertigo can be very effective at relieving vertigo symptoms, but it’s a procedure that should be performed by a physical therapist or other health care professional. This video is for demonstration purposes only. See Doctor Jo’s blog post about the Epley
How to deal with chemical burns and their first aid

some knowledge

Infected Tattoo Abscess
Watch that video to know everything about male and female orgasm
Candidiase Tratamento, Remédio Para Unhas Com Fungos, Fungos Na Pele Como Tratar, Candidíase. http://candidiase-cura.plus101.com/ A intensa existência de substâncias químicas prejudiciais e metais tóxicos em nosso ambiente, nos medicamentos que tomamos, nos alimentos que comemos e até mesmo nos recheios dentários, cria um grande desafio para o nosso corpo se livrar efetivamente dessas toxinas resultando em uma ciclo vicioso que se manifesta em uma variedade de sintomas e problemas de saúde, entre eles é o crescimento excessivo de candida albicans que faz com que os sintomas da infecção por fungos aparecem. A acumulação de metais químicos e tóxicos no interior do corpo também pode levar a desequilíbrios hormonais, alterações genéticas, falhas no sistema imunológico, baixa eliminação, processo de cicatrização mais lenta, problemas de pele, alergias e danos no nervo e no cérebro. A presença de metais pesados ??no corpo (led, prata, mercúrio) proveniente de alimentos, o ar que respiramos, remédios e recheios dentários (contém 50% de amálgama), criam um ambiente ácido e anaeróbio (falta oxigênio) que incentiva a candida sobrecrescimento de fermento. Quando há sobrecarga de metal tóxico no intestino, o revestimento intestinal produz muco extra para impedir que os metais sejam absorvidos na corrente sanguínea. O problema é que esse muco cria um ambiente, que não possui oxigênio, incentivando bactérias e fungos, como organismos como o fermento Candida, a ficarem fora de controle. Além disso, a candida se liga a metais pesados ??(mesmo em seus enchimentos de amálgama) e cresce porque o corpo realiza uma tentativa desesperada de se proteger contra o envenenamento por metais pesados. Uma desintoxicação de metal profundo combinada com a remoção gradual do enchimento dentário de amalgama e substituindo-os por enchimentos brancos mais seguros é uma das etapas mais importantes e fundamentais na luta contra a infecção por levedura de Candida e restabelecendo o equilíbrio do corpo. O Único sistema holístico existente que vai lhe ensinar como curar Permanentemente sua Infecção fúngica, reequilibrar o seu corpo e conseguir a liberdade DURADOURA da Infecção do tipo candidíase! http://candidiase-cura.plus101.com/
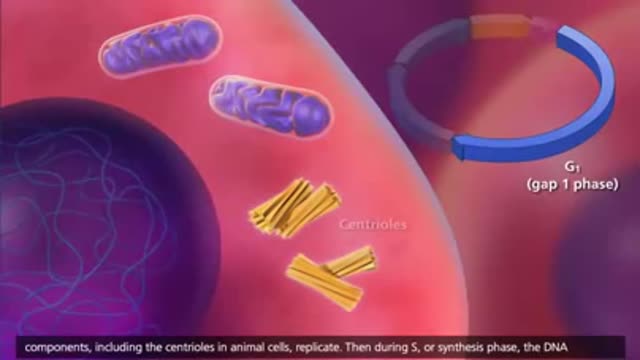
The cell cycle or cell-division cycle is the series of events that take place in a cell leading to its division and duplication of its DNA (DNA replication) to produce two daughter cells.
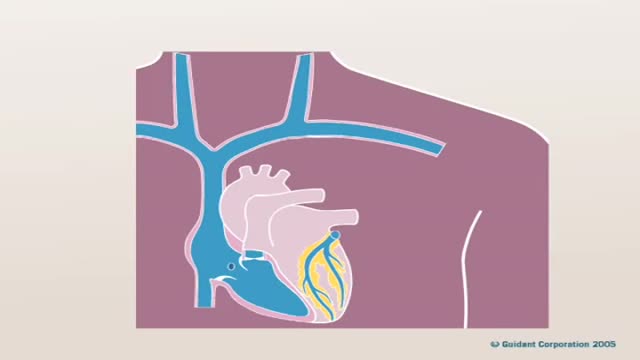
Pacemaker Implantation 3D Animation
Watch that Recto vaginal Exam Video

Physical Examination of the abdomen

Educational video of male patient receiving an anoscopy.

Gastrointestinal GI Drug Delivery

It depends upon which ligament is injured. If it is medial collateral ligament you feel pain when you walk ,sit and stand and you will be liming as well. If it is anterior cruciate ligament you feel pain when you walk on uneven ground.
