- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
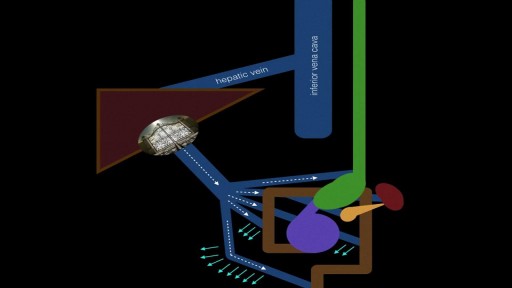
Portal hypertension is an increase in the blood pressure within a system of veins called the portal venous system. ... If the vessels in the liver are blocked due to liver damage, blood cannot flow properly through the liver. As a result, high pressure in the portal system develops
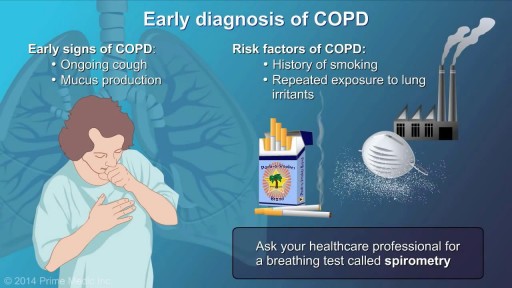
To diagnose COPD, your doctor will probably do the following tests: Medical history and physical exam. These will give your doctor important information about your health. Lung function testsLung function tests, including an FEV1 test. These tests measure the amount of air in your lungs and the speed at which air moves in and out. Spirometry is the most important of these tests. Chest X-rayChest X-ray. This helps rule out other conditions with similar symptoms, such as lung cancer.

Cannula are often introduced into blood vessels in 80% of patients in the hospital for treatment. This can be a daunting experience to patients and stressful to doctors as multiple attempts are used. This may result in introducing spreading MRSA, E Coli & Chlostredium living on your skin into blood and results in Invasive MRSA infection.
Skin is often not adequatly cleaned during subsequent atempts as doctors/nurses do not wait for 1 min after applying cleaning solution on the skin before they puncture your skin.
Multiple punctured sites allow CA-MRSA to enter blood stream resulting in bacteremia and death.
Our mission is to reduce spreading invasive CA-MRSA in the hospitals by developing alternative technique to introduce cannulae.
Medifix was created by doctors with a mission to reduce the threat of spreading antibiotic resustant bacteria to mankind.

Arthrocentesis of the Knee

Surgical Skin Closure Procedures

Watch that video of Pulling Out Teeth Full of Worms and Maggots

This video demonstrates the approach to a large base of tongue tumor, which was invading the ramus of the mandible. The procedure, named after Dr. Trotter, is really a median labiomandibuloglossotomy. In this case this poorly differentiated tumor was resected along with a portion of the floor of mouth. The entire area was reconstructed with a pectoralis major myocutaneous flap.

Demonstration of a one-hand tie for suturing in the operating room.
What is Scleroderma? (also known as Systemic Sclerosis)

Pericardial window is used diagnostically and, more often, therapeutically for drainage of accumulated pericardial fluid (a condition that most often occurs after cardiac surgery but has many other possible causes). The pericardium envelops the heart like a cocoon; its cardiac filling can be impaired when this cavity fills with excess fluid. When the limited space between the noncompliant pericardium and heart is acutely filled with blood or fluid, cardiac compression and tamponade may result. Pericardial window in combination with systemic chemotherapy may also prevent accumulation of large fluid volumes in patients with neoplastic pericardial disease. [1, 2] Indications The following are indications for a pericardial window [6] : Symptomatic pericardial effusions Asymptomatic pericardial effusions that warrant a pericardial window for diagnosis Hemodynamically stable patients with an undiagnosed pericardial effusion (a thoracoscopic approach is ideal) Coexisting pericardial, pleural, or pulmonary pathology that requires diagnosis or therapy (a thoracoscopic approach is ideal) Known benign effusions that reaccumulate after aspiration Drainage of a purulent pericardial effusion Early fungal or tuberculous pericarditis in which resection of the pericardium is required to prevent future pericardial constriction Use as part of the mediastinal debridement, in patients with descending mediastinitis

A chalazion is a swollen bump on the eyelid. It happens when the eyelid’s oil gland clogs up. It may start as an internal hordeolum (stye). At first, you might not know you have a chalazion as there is little or no pain. But as it grows, your eyelid may get red, swollen, and sometimes tender to touch. If the chalazion gets large, it can press on your eye and cause blurry vision. Rarely, the whole eyelid might swell.

Watch that Massive Skin Jiggers Removals

The eyes A close up of a young person's eyes. The eyes are responsible for four-fifths of all the information our brain receives. Here you can find out a bit more about how they work, common problems that affect vision and the work Sightsavers does to treat and prevent avoidable blindness. You can also find out more about the people whose lives have been changed thanks to donations from people like you. How do eyes work? (click image to see enlarged version or click here for text alternative) Graphic of an eye with information about its different parts The images we see are made up of light reflected from the objects we look at. This light enters the eye through the cornea. Because this part of the eye is curved, it bends the light, creating an upside down image on the retina (this is eventually put the right way up by the brain). The retina is a complex part of the eye, but only the very back of it is light sensitive. This part of the retina has roughly the area of a 10p coin, and is packed with photosensitive cells called rods and cones. Cones are the cells responsible for daylight vision. There are three kinds – each responding to a different wavelength of light: red, green and blue. The cones allow us to see images in colour and detail. Rods are responsible for night vision. They are sensitive to light but not to colour. In darkness, the cones do not function at all. How do we see an image? The lens focuses the image. It can do this because it is adjustable – using muscles to change shape and help us focus on objects at different distances. The automatic focusing of the lens is a reflex response and is not controlled by the brain. Once the image is clearly focused on the sensitive part of the retina, energy in the light that makes up that image creates an electrical signal. Nerve impulses can then carry information about that image to the brain through the optic nerve.
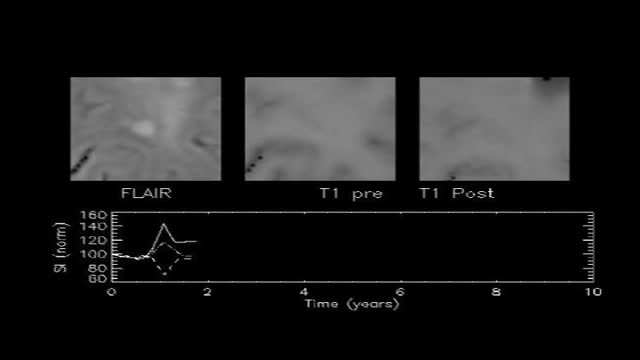
If you have multiple sclerosis (MS), you probably had several tests done before you received your diagnosis. There isn’t one test to diagnosis MS, so testing can vary. Doctors can use neurological exams, information about previous symptoms, blood tests, and spinal fluid tests. A magnetic resonance imaging (MRI) scan isn’t used to diagnose MS but rather to rule out other diseases. A diagnosis of MS requires more information than what a scan alone can give. By looking at more than one test or exam result, doctors can get a clearer picture of what’s going on in your body.
A heart attack is a medical emergency. A heart attack usually occurs when a blood clot blocks blood flow to the heart. Without blood, tissue loses oxygen and dies. Symptoms include tightness or pain in the chest, neck, back, or arms, as well as fatigue, lightheadedness, abnormal heartbeat, and anxiety. Women are more likely to have atypical symptoms than men. Treatment ranges from lifestyle changes and cardiac rehabilitation to medications, stents, and bypass surgery.

Every day, specialists deliver high-quality care in 68 disciplines in health centres across Canada. Yet many Canadians know very little about what many specialists actually do, and the important role these disciplines play in Canada’s health care system.
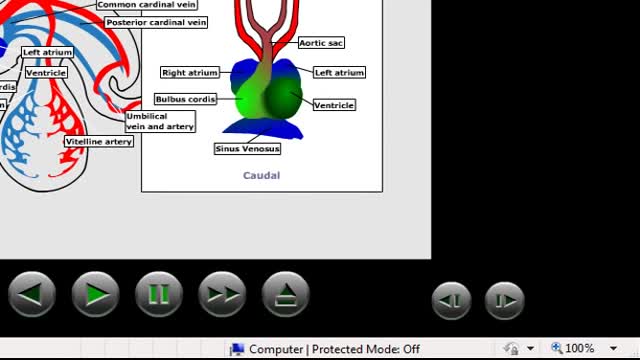
Embryonic cardiovascular system. ... The human arterial and venous systems develop from different embryonic areas. Aortic Arches. The aortic arches—or pharyngeal arch arteries—are a series of six, paired, embryological vascular structures that give rise to several major arteries .

The rotator cuff is a group of muscles and tendons that surround the shoulder joint, keeping the head of your upper arm bone firmly within the shallow socket of the shoulder. A rotator cuff injury can cause a dull ache in the shoulder, which often worsens when you try to sleep on the involved side. Rotator cuff injuries occur most often in people who repeatedly perform overhead motions in their jobs or sports. Examples include painters, carpenters, and people who play baseball or tennis. The risk of rotator cuff injury also increases with age. Many people recover from rotator cuff disease with physical therapy exercises that improve flexibility and strength of the muscles surrounding the shoulder joint. Sometimes, rotator cuff tears may occur as a result of a single injury. In those circumstances, medical care should be provided as soon as possible. Extensive rotator cuff tears may require surgical repair, transfer of alternative tendons or joint replacement.
Human Circulatory System and heart video
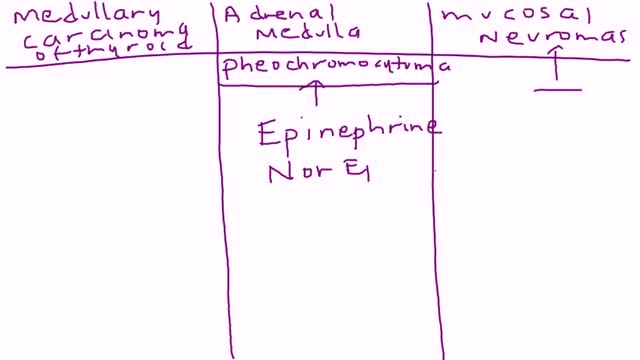
Multiple endocrine neoplasia type 2 (MEN2) is a hereditary condition associated with three primary types of tumors: medullary thyroid cancer, parathyroid tumors, and pheochromocytoma. MEN2 is classified into three subtypes based on clinical features. MEN2A, which affects 60% to 90% of MEN2 families Medullary thyroid cancer: 98% to 100% with MEN2A are affected Pheochromocytoma, a typically benign (noncancerous) tumor of the adrenal glands: 50% with MEN2A affected Parathyroid adenoma (benign tumor) or hyperplasia, meaning increased size, of the parathyroid gland: 5% to 10% with MEN2A affected MEN2B, which affects 5% of MEN2 families Medullary thyroid cancer: 98% to 100% with MEN2B affected Pheochromocytoma: 50% with MEN2B affected Mucosal neuromas, which is a benign tumor of nerve tissue on the tongue, lips and throughout the gastrointestinal tract: 95% to 98% affected Digestive problems caused by disordered nerves in the gastrointestinal tract: 75% to 90% affected Muscle, joint, and spinal problems: 95% affected Typical facial features, including swollen lips and thick eyelids: 75% to 90% affected Familial medullary thyroid cancer (FMTC), which affects 5% to 35% of MEN2 families Medullary thyroid carcinoma only Sources: Gagel RF, Marx SJ. “Multiple endocrine neoplasia.” Williams Textbook of Endocrinology, Chapter 40, 11th ed., Philadelphia, 2008, and Eng C, Clayton D, et al. Grubbs EG, Gagel RF. My, How Things Have Changed in Multiple Endocrine Neoplasia Type 2A! J Clin Endocrinol Metab 100(7):2532-5, 7/2015. PMID: 26151398. What causes MEN2? MEN2 is a genetic condition. This means that the cancer risk and other features of MEN2 can be passed from generation to generation in a family. The gene associated with MEN2 is called RET. A mutation (alteration) in the RET gene gives a person an increased risk of developing medullary thyroid cancer and other tumors associated with MEN2.
