- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
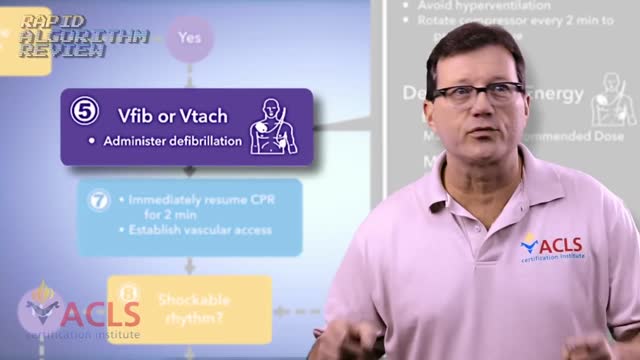
Rapid Algorithm Review Ventricular Fibrillation

ERCP is most commonly performed to diagnose conditions of the pancreas or bile ducts, and is also used to treat those conditions. It is used to evaluate symptoms suggestive of disease in these organs, or to further clarify abnormal results from blood tests or imaging tests such as ultrasound or CT scan. The most common reasons to do ERCP include abdominal pain, weight loss, jaundice (yellowing of the skin), or an ultrasound or CT scan that shows stones or a mass in these organs. ERCP may be used before or after gallbladder surgery to assist in the performance of that operation. Bile duct stones can be diagnosed and removed with an ERCP. Tumors, both cancerous and noncancerous, can be diagnosed and then treated with indwelling plastic tubes that are used to bypass a blockage of the bile duct. Complications from gallbladder surgery can also sometimes be diagnosed and treated with ERCP. In patients with suspected or known pancreatic disease, ERCP will help determine the need for surgery or the best type of surgical procedure to be performed. Occasionally, pancreatic stones can be removed by ERCP.

10 Horrifying Things Found Living Inside a Human Body
You can decrease your risk of getting Lyme disease with some simple precautions: Cover up. ... Use insect repellents. ... Do your best to tick-proof your yard. ... Check yourself, your children and your pets for ticks. ... Don't assume you're immune. ... Remove a tick as soon as possible with tweezers.

Baby Survives Being Born Twice:
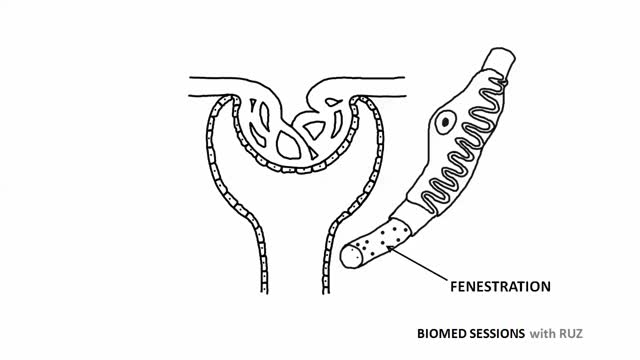
Glomerular filtration is the first step in making urine. It is the process that your kidneys use to filter excess fluid and waste products out of the blood into the urine collecting tubules of the kidney, so they may be eliminated from your body.
Dark Circles around Eyes
HAPPY THANKSGIVING
Alendronate Sodium is used for the following diseases and conditions: osteoporosis, and osteogenesis imperfecta. Alendronate Sodium improves the patient's condition by performing the following functions: slowing down the bone loss and helps to keep the bones strong and less likely to break. Side effects are possible with Alendronate Sodium, but do not always occur. Some of the side effects may be rare but serious. Consult your doctor if you observe any side effects, especially if they do not go away. Alendronate Sodium may cause the following side-effects: stomach pain, constipation, diarrhea, gas, nausea, and jaw pain

What Happens When You're In a Coma?

blood transfusion performance

Chicken Skin Disease, Keratosis Pilaris Lotion, Keratosis Pilaris Laser Treatment, Kp Chicken Skin---- http://banishmybumps.plus101.com/ --- Home Remedies For Keratosis Pilaris. Do you have “chicken skin” that looks like patches on your skin? If yes, you might probably have Keratosis Pilaris. However, do not panic and worry too much. What you should do is to look for the best home remedies for Keratosis Pilaris. But before you proceed with the treatment, you should familiarize yourself on what this skin condition is all about. What is Keratosis Pilaris? Keratosis Pilaris, or KP for short, is an ordinary skin disorder which is characterized by buildup of the tiny bumps in your skin caused by the accretion of keratin inside the follicles of your hair. This benign and non-contagious disorder which can be inherited is also called as “chicken skin”. The Natural Home Cures For Keratosis Pilaris • Regular rubbing of pumice in the inflamed skin part is one from the most efficient natural home cures designed for chicken skin. You could rub a stone when you are already done with foaming. • Use loofah whilst bathing will help you in reducing the visible chicken skin in your body. • Apply an apple cider type of vinegar that is combined with water is also an effective way to get rid of Keratosis Pilaris most especially for children. • Gently rub the granular blend of sugar with two spoonfuls of the sour cream can be used as the simplest herbal home cures for chicken skin. Never use it for children. • Apply yogurt on the inflamed skin and let it stay for 15 until 20 minutes prior to take a shower is also a way on how you can get rid of chicken skin. • You can also use the oil of rose hip or any oil that contains vitamin E and apply it towards the inflamed area. While you are following these home remedies for Keratosis Pilaris, refrain from scrubbing the inflamed skin part vigorously because this can promote irritation on the follicles of your hair. Besides, whenever taking a bath or shower, never use very hot water to avoid drying and roughing of the skin. This could also make the problem worsen. Managing your KP may seem like a winless battle, but there is good news. Recent research has shown that all-natural treatment options, including BanishMyBumps, are successful at stopping keratosis pilaris in its tracks. Learn more at http://banishmybumps.plus101.com/

baby wrapping
Como Mantener Una Erección, Vitaminas Para Hombre, Remedio Para Impotencia Masculina.--- http://erecciones-increibles.good-info.co --- Por qué los medicamentos para la disfunción eréctil no son la respuesta, Probablemente has visto los comerciales de Viagra, Cialis, y los otros medicamentos populares utilizados en el tratamiento de la disfunción eréctil. Las grandes empresas farmacéuticas están constantemente bombardeando con anuncios, tanto en la televisión y en línea, exagerando los beneficios de su clase más reciente de "medicamentos maravillosos". Son tan populares que muchas personas que ni siguiera tienen disfunción eréctil tratan de conseguir algunas de las pastillas para un "uso recreativo" ocasional. ¿Alguna vez te has preguntado por qué las empresas farmacéuticas apuntarían a TI en sus anuncios? Después de todo, no puedes conseguir estos medicamentos sin receta, así que mostrarte un anuncio sobre estas drogas parece ilógico. Pero cuando lo piensas, comienza a tener más sentido... La primera vez que empieces a experimentar problemas con tu desempeño sexual, es casi seguro que le pedirás a tu doctor una de las drogas que has visto en TV. Entonces, por supuesto, una vez que ves que la " pastilla mágica" funciona para ti, estás enganchado. ¡Tienen un nuevo cliente de por vida! El problema verdadero aquí es que las grandes compañías farmacéuticas NO tienen absolutamente ningún interés en curarte de la disfunción eréctil. Prefieren ver que estás enganchado en su medicamento muy costoso para siempre. Esos son ingresos mensuales garantizados para ellos, pero para ti, no es una cura, sino una solución alternativa y una carga financiera. No cometas el error de pensar que los tratamientos para disfunción eréctil son la única clase de medicamento con los que hacer esto. Las grandes farmacéuticas están en el negocio de vender soluciones temporales en lugar de curas permanentes. Esta es la única cura comprobada para la disfunción eréctil que es 100% segura y natural, y combina un secreto ancestral de los amantes más viriles del mundo con ciencia moderna y revolucionaria… Ingresa ahora a: http://erecciones-increibles.good-info.co

Que Es Bueno Para La Impotencia Del Hombre, Problemas Para Mantener La Erección, Que Es Erección.--- http://erecciones-increibles.good-info.co --- 5 Errores comunes que empeoran tu disfunción eréctil, Cuando se trata de problemas de salud, a menudo somos nuestros peores enemigos. Esto se ve en muchos casos y con una variedad de enfermedades. Las personas que saben que tienen la presión arterial elevada y colesterol alto no cambian su dieta y siguen comiendo un montón de comida frita, por ejemplo. La disfunción eréctil no es diferente. Aquí hay cinco cosas que podrías estar haciendo en este momento, hoy, que están empeorando tu estado. Estás comiendo (y bebiendo) cosas malas Cafeína. Alcohol. Nicotina. Drogas. Exceso de grasa. Si disfrutas de cualquiera de estas cosas habitualmente, la triste verdad es que estás empeorando tu disfunción eréctil. Incluso si haces otras cosas para mejorar tu estado - incluso si tomas medicación para compensarlo, esas cosas serán menos eficaces de lo que podrían ser a menos que reduzcas dramáticamente o elimines los ítems mencionados anteriormente. No estás comiendo suficiente cosas buenas A continuación se presenta una corta lista de alimentos para aumentar tu salud vascular, lo que a su vez, mejorará la calidad de tus erecciones: granos enteros, verduras de hojas verdes, frutas (especialmente la sandía y arándanos), y ostras. Si te gusta todo lo de esa lista, estás de suerte. Come más de todo eso y vas a ver que los síntomas de la disfunción eréctil disminuyen considerablemente, y posiblemente incluso desaparezcan. Si actualmente no estás comiendo ninguno de los anteriormente, entonces definitivamente estás empeorando el problema. En sí misma, la dieta puede no ser completamente capaz de curar tu disfunción eréctil, pero puede hacer una gran diferencia y tener un tremendo impacto en la calidad de tus erecciones. Esta es la única cura comprobada para la disfunción eréctil que es 100% segura y natural, y combina un secreto ancestral de los amantes más viriles del mundo con ciencia moderna y revolucionaria… Ingresa ahora a: http://erecciones-increibles.good-info.co

Watch that video to see how black salve left inch-wide hole in man's face

Watch that video of Huge Foot blister Freezing With Liquid Nitrogen
Regime Rapide, Perdre De La Graisse, Rajeunissement, Corps Neuf, Exercices Pour Perdre Du Poids ---- http://rajeunir-de-10-ans.info-pro.co --- Pourquoi vous ne devriez jamais vous entraîner plus de 90 minutes par semaine Saviez-vous que vous entraîner plus de 90 minutes par semaine peut accélérer le vieillissement de votre corps plus rapidement? Cet article de mon copain Steve Holman explique exactement pourquoi: http://rajeunir-de-10-ans.info-pro.co Dans l'article, il partage également avec vous cinq techniques bizarres pour paraître dix ans plus jeune ... des choses étonnantes dont vous n'avez probablement jamais entendu parler auparavant. Vérifiez les ici: http://rajeunir-de-10-ans.info-pro.co Les dangers de TROP faire d'exercices! Dans l'article, il partage également avec vous 5 façons uniques pour paraître dix ans plus jeune ... des choses étonnantes dont vous n'avez probablement jamais entendu parler auparavant. Vérifiez- les ici: http://rajeunir-de-10-ans.info-pro.co 5 façons uniques pour paraître dix ans plus jeune (et les dangers de faire trop d'exercice) Les 5 étapes pour Rajeunir de 10 ans! Cliquez Ici: http://rajeunir-de-10-ans.info-pro.co

Manipulation L5/S1 Lumbar Roll and Sacroiliac joint Sidelying

