- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

For those that aren't good LASIK candidates, PRK is a procedure that offers the same great results! Watch Dr. Ferguson explain each step during Samantha's procedure. Her reaction at the end is incredible!

From UW Health's Neurosurgery Program: Learn more about the individual steps in the DBS surgery procedure. Visit uwhealth.org/dbs

A brain surgery called a craniectomy is performed to remove a part of your skull in order to relieve pressure in an area when your brain swells from a traumatic brain injury. It is also performed to treat medical conditions that cause your brain to swell or bleed that can be caused by an aneurysm, brain tumor or other cancer.
This 3d animation shows how the surgical procedure decreases intracranial pressure (ICP), intracranial hypertension (ICHT), or heavy bleeding (also called hemorrhaging) inside your skull. If left untreated, pressure or bleeding can compress your brain and push it down onto the brain stem. This can be fatal or cause permanent brain damage.
Brain surgery is a very serious procedure under any circumstances, but a craniectomy is done when there is an immediate risk to the brain and neurological function due to severe brain injury or stroke.
For more information about custom 3D animation depicting surgery, please visit https://www.amerra.com/.
Watch additional medical animations:
Accessing an implantable port training - 3D animation: https://youtu.be/xSTpxjyv4O4
Open Suctioning with a Tracheostomy Tube - 3D animation: https://youtu.be/wamB7jpWCiQ
Ventriculostomy Brain Surgery - 3d animation: https://youtu.be/pUy0YDzVNzs
Suctioning the endotracheal tube - medical animation: https://youtu.be/pN6-EYoeh3g
Functional endoscopic sinus surgery (FESS) - 3D animation: https://youtu.be/qKTRyowwaLA
How to insert a nasogastric tube for NG intubation - 3d animation: https://youtu.be/Abf3Gd6AaZQ
Oral airway insertion - oropharyngeal airway technique - 3D animation: https://youtu.be/caxUdNwjt34
Nasotracheal suctioning (NTS) - 3D animation: https://youtu.be/979jWMsF62c
Learn about hemorrhoids with #3d #animation: https://youtu.be/R6NqlMpsiiY
LASIK eye surgery - 3D animation: https://youtu.be/Bb8bnjnEM00
CPR cardiopulmonary resuscitation - 3D animation: https://youtu.be/G87knTZnhks
What are warts (HPV)? - 3D animation: https://youtu.be/guJ1J7rRs1w
How Macular Degeneration Affects Your Vision - 3D animation: https://youtu.be/ozZQIZ_52YY
NeoGraft hair transplant procedure – animation: https://youtu.be/C-eTdH2UPXI
Dr. Horacio Asbun, Mayo Clinic in Florida, explains the Whipple procedure using this animated graphic of a pancreas. Cancer of the pancreas affects 45,000 people every year in the U.S., and it is the fourth leading cause of cancer-related deaths. The five-year overall survival rate if a tumor is detected early and surgically removed is 22 percent, versus 6 percent without early detection and surgery. To learn more, visit http://mayocl.in/2zk7FDi.
This video in Spanish/español: https://www.youtube.com/watch?v=N_zWboNMKWk

Cleft palate is among the most common birth defects affecting children in North America. The incomplete formation of the roof of the mouth can occur individually, or in addition to cleft lip. Cleft palate repair is a type of plastic surgery to correct this abnormal development both to restore function and a more normal appearance. This video explains what to expect for families scheduled for cleft palate surgery at the Craniofacial Anomalies Program at University of Michigan C.S. Mott Children's Hospital.
Learn more about our program at http://www.mottchildren.org/craniofacial

Learn Basic Laparoscopic Surgery, the components of a laparoscopic surgical setup, optimal positioning and ergonomics in laparoscopic surgery, and much more. Check out the full course for free here: https://www.incision.care/free-trial
What is Laparoscopic Surgery:
Laparoscopic surgery describes procedures performed using one or multiple small incisions in the abdominal wall in contrast to the larger, normally singular incision of laparotomy. The technique is based around principles of minimally invasive surgery (or minimal access surgery): a large group of modern surgical procedures carried out by entering the body with the smallest possible damage to tissues. In abdominopelvic surgery, minimally invasive surgery is generally treated as synonymous with laparoscopic surgery as are procedures not technically within the peritoneal cavity, such as totally extraperitoneal hernia repair, or extending beyond the abdomen, such as thoraco-laparoscopic esophagectomy. The term laparoscopy is sometimes used interchangeably, although this is often reserved to describe a visual examination of the peritoneal cavity or the purely scopic component of a laparoscopic procedure. The colloquial keyhole surgery is common in non-medical usage.
Surgical Objective of Laparoscopic Surgery:
The objective of a laparoscopic approach is to minimize surgical trauma when operating on abdominal or pelvic structures. When correctly indicated and performed, this can result in smaller scars, reduced postoperative morbidity, shorter inpatient durations, and a faster return to normal activity. For a number of abdominopelvic procedures, a laparoscopic approach is now generally considered to be the gold-standard treatment option.
Definitions
Developments of Laparoscopic Surgery:
Following a number of smaller-scale applications of minimally invasive techniques to abdominopelvic surgery, laparoscopic surgery became a major part of general surgical practice with the introduction of laparoscopic cholecystectomy in the 1980s and the subsequent pioneering of endoscopic camera technology. This led to the widespread adoption of the technique by the early- to mid-1990s. The portfolio of procedures that can be performed laparoscopically has rapidly expanded with improvements in instruments, imaging, techniques and training — forming a central component of modern surgical practice and cross-specialty curricula [2]. Techniques such as laparoscopically assisted surgery and hand-assisted laparoscopic surgery have allowed the application of laparoscopic techniques to a greater variety of pathology. Single-incision laparoscopic surgery, natural orifice transluminal endoscopic surgery, and minilaparoscopy-assisted natural orifice surgery continue to push forward the applications of minimally invasive abdominopelvic techniques; however, the widespread practice and specific indications for these remain to be fully established. More recently, robotic surgery has been able to build on laparoscopic principles through developments in visualization, ergonomics, and instrumentation.
This Basic Laparoscopic Surgery Course Will Teach You:
- Abdominal access techniques and the different ways of establishing a pneumoperitoneum
- Principles of port placement and organization of the operative field
- Key elements of laparoscopic suturing, basic knotting and clip application
Specific attention is paid to the following hazards you may encounter:
- Fire hazard and thermal injury
- Lens fogging
- Contamination of insufflation system
- Complications from trocar introduction
- Limitations of Veress needle technique
- Limitations of open introduction technique
- Complications of the pneumoperitoneum
- Gas embolism
- Mirroring and scaling of instrument movements
- Firing clip applier without a loaded clip
The following tips are designed to improve your understanding and performance:
- Anatomy of a laparoscope
- Checking for optic fiber damage
- "White balance" of camera
- Checking integrity of electrosurgical insulation
- Access at Palmer's point
- Lifting abdominal wall before introduction
- Confirming position of Veress needle
- Umbilical anatomy
- Identification of inferior epigastric vessels under direct vision
- Translumination of superficial epigastric vessels
- Selection of trocar size
- Aiming of trocar
- Working angles in laparoscopic surgery
- Choice of suture material
- Instruments for suturing
- Optimal ergonomics for suturing
- Extracorporeal needle positioning
- Optimal suture lengths
- "Backloading" needle
- Intracorporeal needle positioning
- Hand movements when suturing
- Optimal positioning of scissors
- Extracorporeal knot tying
- Visualization of clip applier around target structure
- Common clip configurations

This video demonstrates a manual small incision cataract surgery using a Blumenthal technique, in a white cataract.
Surgeon: Dr. Rishi Swarup, FRCS, Medical Director & Senior Consultant, Swarup Eye Centre, India

Dr. Debbie Song at Gillette Children's describes in detail selective rhizotomy surgery.
A selective dorsal rhizotomy is an operation performed to treat spasticity. It is thought that high tone and spasticity arise from abnormal signals that are transmitted through sensory or dorsal nerve roots to the spinal cord. In a selective dorsal rhizotomy we identify and cut portions of the dorsal nerve roots that carry abnormal signals thereby disrupting the mechanisms that lead to spasticity. Potential patients go through a rigorous assessment that includes an in-depth gait and motion analysis as well as a physical therapy evaluation.
They are evaluated by a multidisciplinary team that includes a pediatric rehabilitation doctor, a neurosurgeon, and an orthopedist, Appropriate patient selection is vital. Ideal candidates for selective dorsal rhizotomy are children who are between four and ten years of age, have a history of being born prematurely, and have a diagnosis of diplegia cerebral palsy. These patients usually walk independently or with the assistance of crutches or a walker. They typically function at a level one, two, or three in the gross motor function classification system or gmfcs. A selective dorsal rhizotomy involves the coordinated efforts of the neurosurgery, physiatry, anesthesia and nursing teams. The operation entails making an incision in the lower back that is approximately six to eight inches long. We perform what we call a laminoplasty in which we remove the back part of the spinal elements from the lumbar one or l1 to l5 levels. At the end of the procedure the bone is put back on. We identify and open up the Dural sac that contain the spinal fluid spinal cord and nerve roots. Once the Dural sac is opened ,we expose the lumbar and upper sacral nerve roots that transmit information to and from the muscles of the lower extremities.
At each level we isolate the dorsal nerve root, which in turn is separated into as many as 30 smaller thread light fruitlets.
Each rootlet is then electrically stimulated. Specialized members of the physiatry team look for abnormal responses in the muscles of the legs as each rootless is being stimulated. If an abnormal response is observed then the rootlet is cut.
If a normal response is observed, then the rootlet is not cut. We usually end up cutting approximately 20 to 40 percent of the rootlets. The Dural sac is sutured closed and the l1 through l5 spinal elements are put back into anatomic position, thus restoring normal spinal alignment. The overlying tissues and skin are then closed and the patient is awoken from surgery. The entire operation takes between four and five hours. A crucial component to the success of our rhizotomy program is the extensive rehabilitation course following surgery. With their tone significantly reduced after a rhizotomy, patients relearn how to use their muscles to walk more efficiently through stretching, strengthening, and gait training. Approximately one to two years after a rhizotomy patients undergo repeat gait and motion analysis. The orthopedic surgeons assess the need for interventions to correct bone deformities, muscle contractures, poor motor control, impaired balance, or other problems related to cerebral palsy.
At Gillette we work closely with patients and families to ensure that our selective dorsal rhizotomy program meets their goals for enhancing their function and improving their quality of life.
VISIT https://www.gillettechildrens.org/ to learn more
0:00 Why choose selective dorsal rhizotomy?
0:56 Who is a good candidate for selective dorsal rhizotomy?
1:31 What does a selective dorsal rhizotomy entail?
3:26 What is recovery from selective dorsal rhizotomy like?

For more information about Mohs surgery, please visit https://cle.clinic/3x7CRTy
Mohs surgery is a highly effective skin cancer removal procedure that takes just a few hours. It is most often used to treat basal cell and squamous cell carcinomas, the two most common skin cancers.
Chapters:
0:00 How effective is Mohs Surgery?
0:23 When is Mohs Surgery used?
0:50 How does Mohs Surgery work?
1:55 Does Mohs Surgery cure skin cancer?
2:06 How long is the recovery period after Mohs Surgery?
Resources:
Skins Cancer: https://cle.clinic/3G2MMM8
How Skin Cancer Is Found and Removed — At the Same Appointment: https://cle.clinic/3r9Wzu6
The Best Strategies To Reduce Your Risk of Skin Cancer: https://cle.clinic/38Bazqn
The information in this video was accurate as of 4.8.2022 and is for information purposes only. Consult your local medical authority or your healthcare practitioner for advice.
▶Share this video with others: https://youtu.be/aCV1UZ0Yj-o
▶Subscribe to learn more about Cleveland Clinic:
https://www.youtube.com/user/C....levelandClinic?sub_c
#ClevelandClinic #MohsSurgery #SkinCancer

Christopher J. Rapuano, MD, Director of the Cornea Service at Wills Eye Institute describes his surgical approach of a Combined Penetrating Keratoplasty (PK) and Cataract Surgery
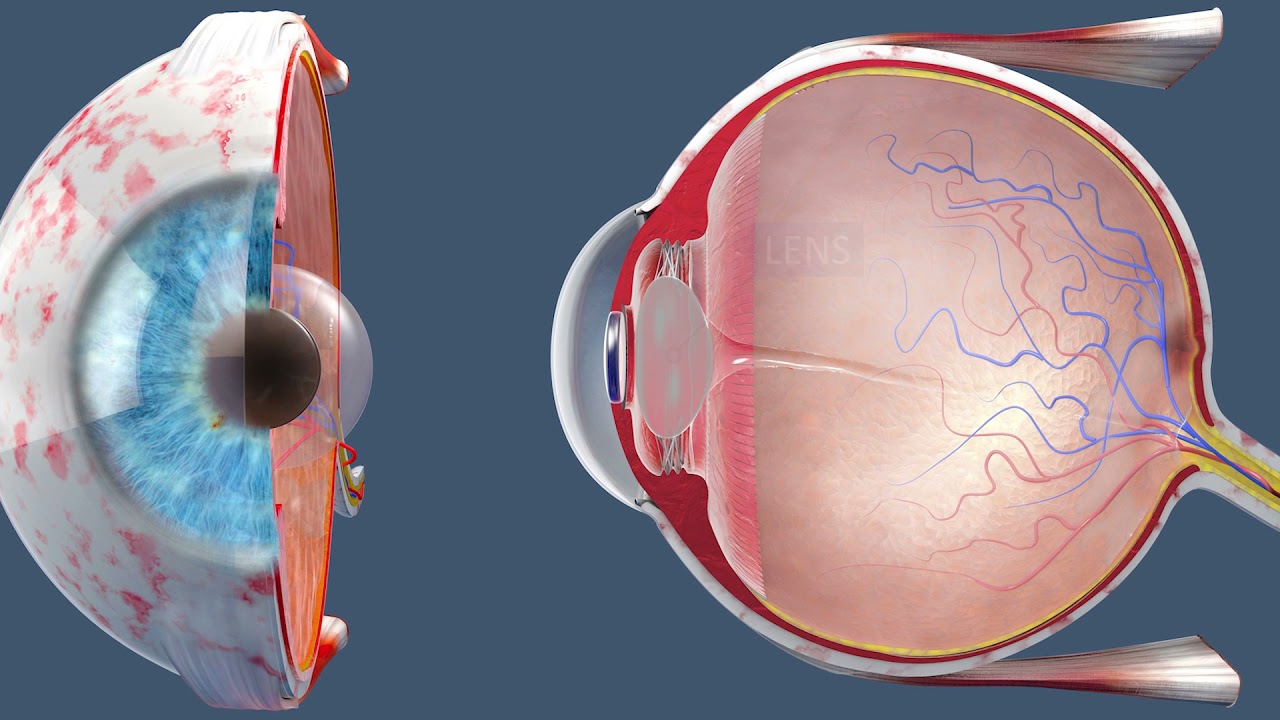
The patient is awake as a laser cuts her cataract into six pieces. Then, she heads into the operating room. When she wakes up, her cataracts and nearsightedness are gone.
#insidetheor

The video demonstrates complete excision of endometrosis in a variety of challenging situations.

.
Chapters
0:00 Introduction
1:04 Why do doctors perform laparoscopy?
2:11 How is laparoscopy performed?
3:22 Result
3:47 Risk of laparoscopy
Laparoscopy (from Ancient Greek λαπάρα (lapára) 'flank, side', and σκοπέω (skopéō) 'to see') is an operation performed in the abdomen or pelvis using small incisions (usually 0.5–1.5 cm) with the aid of a camera. The laparoscope aids diagnosis or therapeutic interventions with a few small cuts in the abdomen.[1]
Laparoscopic surgery, also called minimally invasive procedure, bandaid surgery, or keyhole surgery, is a modern surgical technique. There are a number of advantages to the patient with laparoscopic surgery versus an exploratory laparotomy. These include reduced pain due to smaller incisions, reduced hemorrhaging, and shorter recovery time. The key element is the use of a laparoscope, a long fiber optic cable system that allows viewing of the affected area by snaking the cable from a more distant, but more easily accessible location.
Laparoscopic surgery includes operations within the abdominal or pelvic cavities, whereas keyhole surgery performed on the thoracic or chest cavity is called thoracoscopic surgery. Specific surgical instruments used in laparoscopic surgery include obstetrical forceps, scissors, probes, dissectors, hooks, and retractors. Laparoscopic and thoracoscopic surgery belong to the broader field of endoscopy. The first laparoscopic procedure was performed by German surgeon Georg Kelling in 1901. There are two types of laparoscope:[2]
A telescopic rod lens system, usually connected to a video camera (single-chip or three-chip)
A digital laparoscope where a miniature digital video camera is placed at the end of the laparoscope, eliminating the rod lens system
The mechanism mentioned in the second type is mainly used to improve the image quality of flexible endoscopes, replacing conventional fiberscopes. Nevertheless, laparoscopes are rigid endoscopes. Rigidity is required in clinical practice. The rod-lens-based laparoscopes dominate overwhelmingly in practice, due to their fine optical resolution (50 µm typically, dependent on the aperture size used in the objective lens), and the image quality can be better than that of the digital camera if necessary. The second type of laparoscope is very rare in the laparoscope market and in hospitals.[citation needed]
Also attached is a fiber optic cable system connected to a "cold" light source (halogen or xenon) to illuminate the operative field, which is inserted through a 5 mm or 10 mm cannula or trocar. The abdomen is usually insufflated with carbon dioxide gas. This elevates the abdominal wall above the internal organs to create a working and viewing space. CO2 is used because it is common to the human body and can be absorbed by tissue and removed by the respiratory system. It is also non-flammable, which is important because electrosurgical devices are commonly used in laparoscopic procedures.[3]
Procedures
Surgeons perform laparoscopic stomach surgery.
Patient position
During the laparoscopic procedure, the position of the patient is either in Trendelenburg position or in reverse Trendelenburg. These positions have an effect on cardiopulmonary function. In Trendelenburg's position, there is an increased preload due to an increase in the venous return from lower extremities. This position results in cephalic shifting of the viscera, which accentuates the pressure on the diaphragm. In the case of reverse Trendelenburg position, pulmonary function tends to improve as there is a caudal shifting of viscera, which improves tidal volume by a decrease in the pressure on the diaphragm. This position also decreases the preload on the heart and causes a decrease in the venous return leading to hypotension. The pooling of blood in the lower extremities increases the stasis and predisposes the patient to develop deep vein thrombosis (DVT).[4]
Gallbladder
Rather than a minimum 20 cm incision as in traditional (open) cholecystectomy, four incisions of 0.5–1.0 cm, or more recently, a single incision of 1.5–2.0 cm,[5] will be sufficient to perform a laparoscopic removal of a gallbladder. Since the gallbladder is similar to a small balloon that stores and releases bile, it can usually be removed from the abdomen by suctioning out the bile and then removing the deflated gallbladder through the 1 cm incision at the patient's navel. The length of postoperative stay in the hospital is minimal, and same-day discharges are possible in cases of early morning procedures.[citation needed]
Colon and kidney
Dr. Celia Divino, Chief, Division of General Surgery at The Mount Sinai Hospital, performs a laparoscopic appendectomy. Visit the Division of General Surgery at http://bit.ly/18z944M. Click here to learn more about Dr. Celia Divino http://bit.ly/12RF0ee

This Basic Laparoscopic Surgery: Abdominal Access and Trocar Introduction course will teach you the steps of Laparoscopic Surgery. View the full course for free by signing up on our website: https://www.incision.care/
What is Laparoscopic Surgery:
Laparoscopic surgery describes procedures performed using one or multiple small incisions in the abdominal wall in contrast to the larger, normally singular incision of laparotomy. The technique is based around principles of minimally invasive surgery (or minimal access surgery): a large group of modern surgical procedures carried out by entering the body with the smallest possible damage to tissues. In abdominopelvic surgery, minimally invasive surgery is generally treated as synonymous with laparoscopic surgery as are procedures not technically within the peritoneal cavity, such as totally extraperitoneal hernia repair, or extending beyond the abdomen, such as thoraco-laparoscopic esophagectomy. The term laparoscopy is sometimes used interchangeably, although this is often reserved to describe a visual examination of the peritoneal cavity or the purely scopic component of a laparoscopic procedure. The colloquial keyhole surgery is common in non-medical usage.
Surgical Objective of Laparoscopic Surgery:
The objective of a laparoscopic approach is to minimize surgical trauma when operating on abdominal or pelvic structures. When correctly indicated and performed, this can result in smaller scars, reduced postoperative morbidity, shorter inpatient durations, and a faster return to normal activity. For a number of abdominopelvic procedures, a laparoscopic approach is now generally considered to be the gold-standard treatment option.
Definitions
Developments of Laparoscopic Surgery:
Following a number of smaller-scale applications of minimally invasive techniques to abdominopelvic surgery, laparoscopic surgery became a major part of general surgical practice with the introduction of laparoscopic cholecystectomy in the 1980s and the subsequent pioneering of endoscopic camera technology. This led to the widespread adoption of the technique by the early- to mid-1990s. The portfolio of procedures that can be performed laparoscopically has rapidly expanded with improvements in instruments, imaging, techniques and training — forming a central component of modern surgical practice and cross-specialty curricula [2]. Techniques such as laparoscopically assisted surgery and hand-assisted laparoscopic surgery have allowed the application of laparoscopic techniques to a greater variety of pathology. Single-incision laparoscopic surgery, natural orifice transluminal endoscopic surgery, and minilaparoscopy-assisted natural orifice surgery continue to push forward the applications of minimally invasive abdominopelvic techniques; however, the widespread practice and specific indications for these remain to be fully established. More recently, robotic surgery has been able to build on laparoscopic principles through developments in visualization, ergonomics, and instrumentation.
This Basic Laparoscopic Surgery: Abdominal Access and Trocar Introduction course will teach you:
- How to access the abdomen using an open, closed, and direct optical-entry technique
- Principles underlying safe abdominal insufflation
- The vascular anatomy of the abdominal wall and its implications for trocar placement
- How to introduce trocars into the peritoneal cavity
- The principle of triangulation and how this can be applied to organizing a laparoscopic surgical field
Specific attention is given to these hazards you may encounter:
- Intravascular, intraluminal, or extraperitoneal needle position
- Limitations of a closed introduction technique
- Abdominal surgical history
- Limitations of an open introduction technique
- Optical trocar entry in thin individuals
- Visualization of non-midline structures
- Limitations of direct optical-entry techniques
- Limitations of clinical examination to confirm intraperitoneal insufflation
- Leakage of insufflation gas
These tips are designed to help you improve your understanding and performance:
- Alternative left upper quadrant approach
- Testing Veress needle before use
- Lifting the abdominal wall for Veress needle introduction
- "Hanging-drop test"
- Palmer's test
- Confirming intra-abdominal insufflation
- Subcutaneous tissue retraction
- Anatomy of the umbilicus
- Retraction of abdominal wall fascia
- Finger sweep of anterior abdominal wall
- Lifting the abdominal wall for optical trocar introduction
- Identification of venous bleeding at the end of a procedure
- Identification of inferior epigastric vessels by direct vision
- Peritoneal folds of the anterior abdominal wall
- Transillumination of superficial epigastric vessels
- Infiltration of local anesthetic at port sites
- Aiming of trocars
- Selection of trocar size
- Maintaining direct vision

OB_A_1013
3D animation depicting the operating room and initial procedure preparing the patient for a laparoscopic hysterectomy. The patient is prepped and draped in the usual fashion and surrounded by the surgeon and surgical assistants. The skin is elevated, an infraumbilical incision is made, a trocar port is inserted through the incision and the abdomen is insufflated. Finally, a laparoscope is inserted into the port to allow for direct visualization of the uterus and the surgery can begin.
To view more animations and exhibits, visit our medical library: https://www.trialexhibitsinc.c....om/library/multimedi
Contact us on your next case for consulting, trial graphics, animations, medical illustrations or presentation services. 800-591-1123 [a]www.trialex.com[/a]
This video is for reference only. The video may not be otherwise used, reproduced nor modified. For more information to purchase a copy or permission to use this animation on your next case, project, website or TV, contact us at [a]www.trialex.com[/a] or 800-591-1123.
Copyright @ Trial Exhibits, Inc.

UChicago Medicine organ transplant surgeon Dr. Rolf Barth explains a how the laparoscopic donor nephrectomy – also known as the single-port nephrectomy – procedure works to remove an organ donor’s kidney from their body to be transplanted into a recipient. This minimally invasive kidney donor transplant surgery allows living organ donors the get back to their lives more quickly than the traditional approach and leaves them with a nearly invisible scar in the belly button.
Learn more about living kidney donation: https://www.uchicagomedicine.o....rg/conditions-servic

Visit our website to learn more about using Nucleus animations for patient engagement and content marketing: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=appendect-020615
This 3D medical animation depicts the surgical removal of the appendix (appendectomy) using laparoscopic instruments. The surgery animation begins by showing an inflamed appendix (appendicitis), followed by the placement of the laparoscope. Afterward, one can see the surgical device staple, cut and remove the inflamed appendix. Following the removal of the appendix the abdomen is flushed with a sterile saline solution to ensure all traces of infection have been removed.
#laparoscopy #appendix #appendicitis
ANCE00183
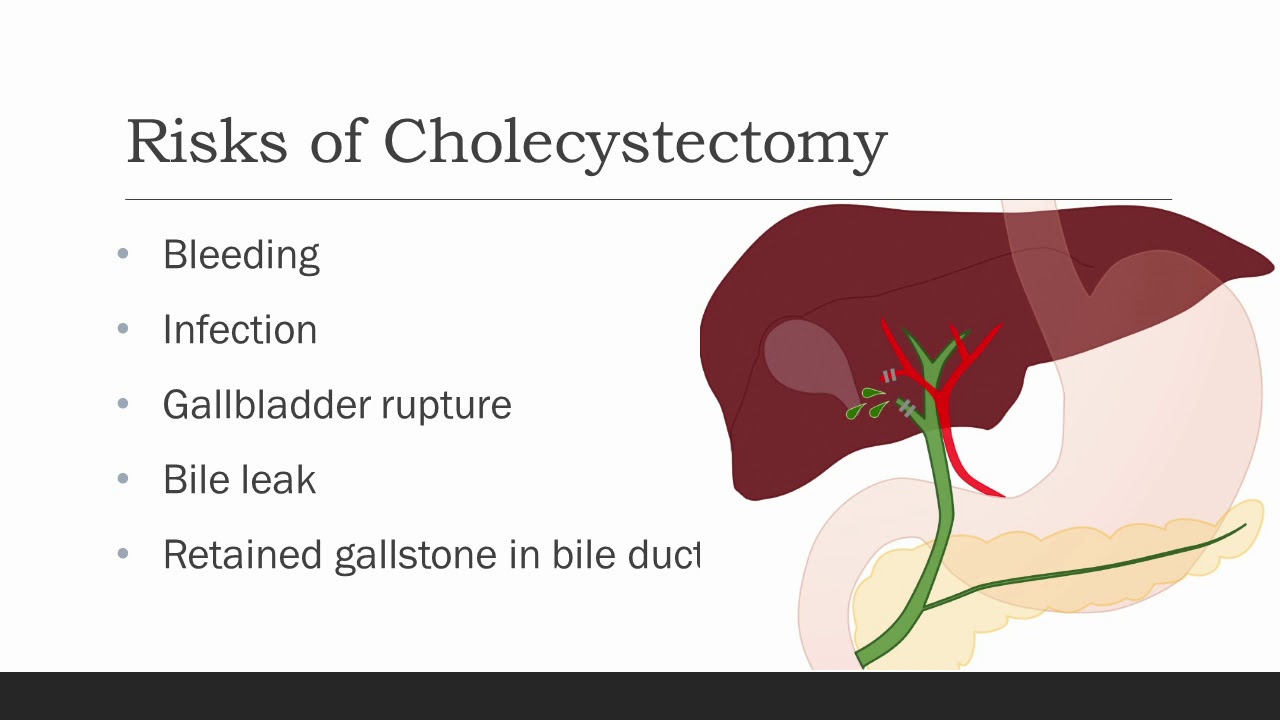
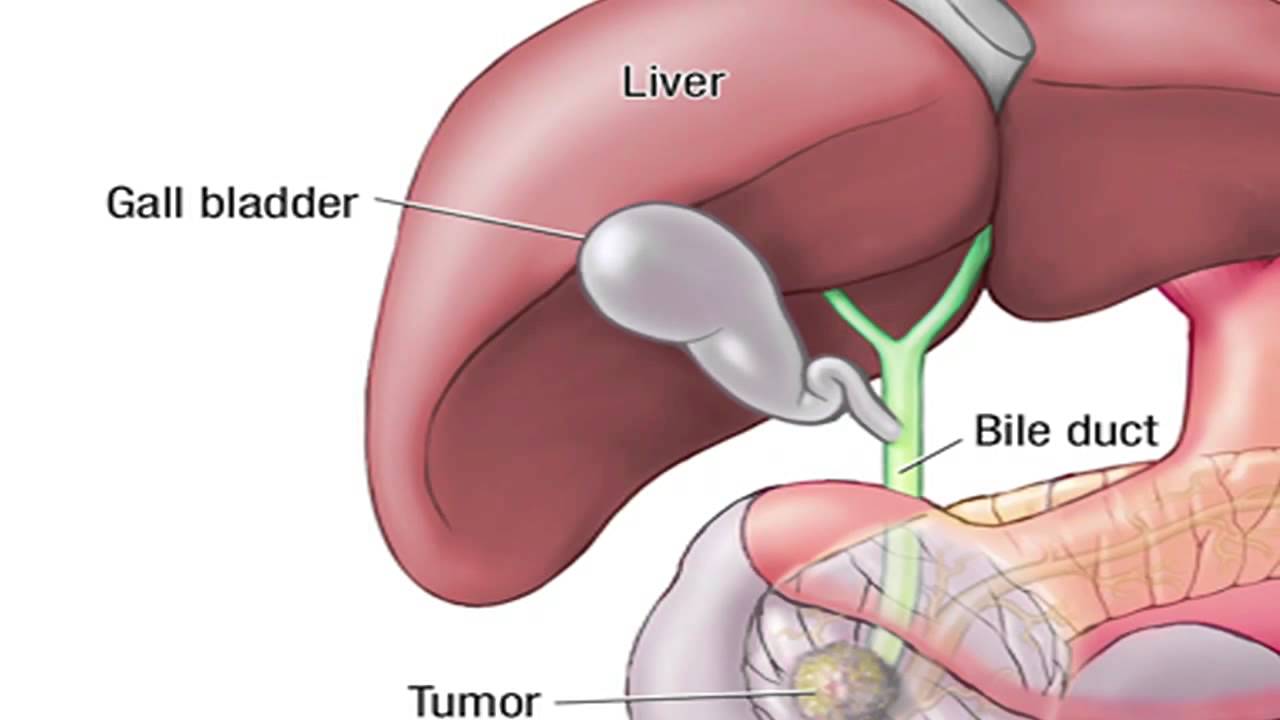
Cholecystectomy means removal of the gallbladder. The most common reasons
your doctor might recommend a cholecystectomy are biliary colic, cholecystitis,
choledocolithiasis, or gallstone pancreatitis. Biliary colic, also known as symptomatic
cholelithiasis, is caused by gallstones, which are hardened deposits of bile. Gallstones are
common in the general population, and gallstones alone are not a reason for gallbladder
removal if they do not cause symptoms. However, sometimes gallstones can get caught at the
neck of the gallbladder, causing pain when the gallbladder contracts against them trying to
release its bile, especially after a fatty meal. With biliary colic, the pain typically resolves within
an hour or so. Occasionally, a stone or some other blockage may prevent the gallbladder from
emptying over a long period of time, causing an increase in pressure and trapped fluid within the
gallbladder. This can cause inflammation and infection of the gallbladder, which we call
cholecystitis. Choledocholithiasis is when there are one or more stones in the bile ducts, which
can cause back up of bile into the liver, and depending on the location of the stones, could
cause pancreatitis, which is inflammation of the pancreas. Other reasons for gallbladder
removal, though less common, are gallbladder polyps and cancer. All of these are reasons for
gallbladder removal.

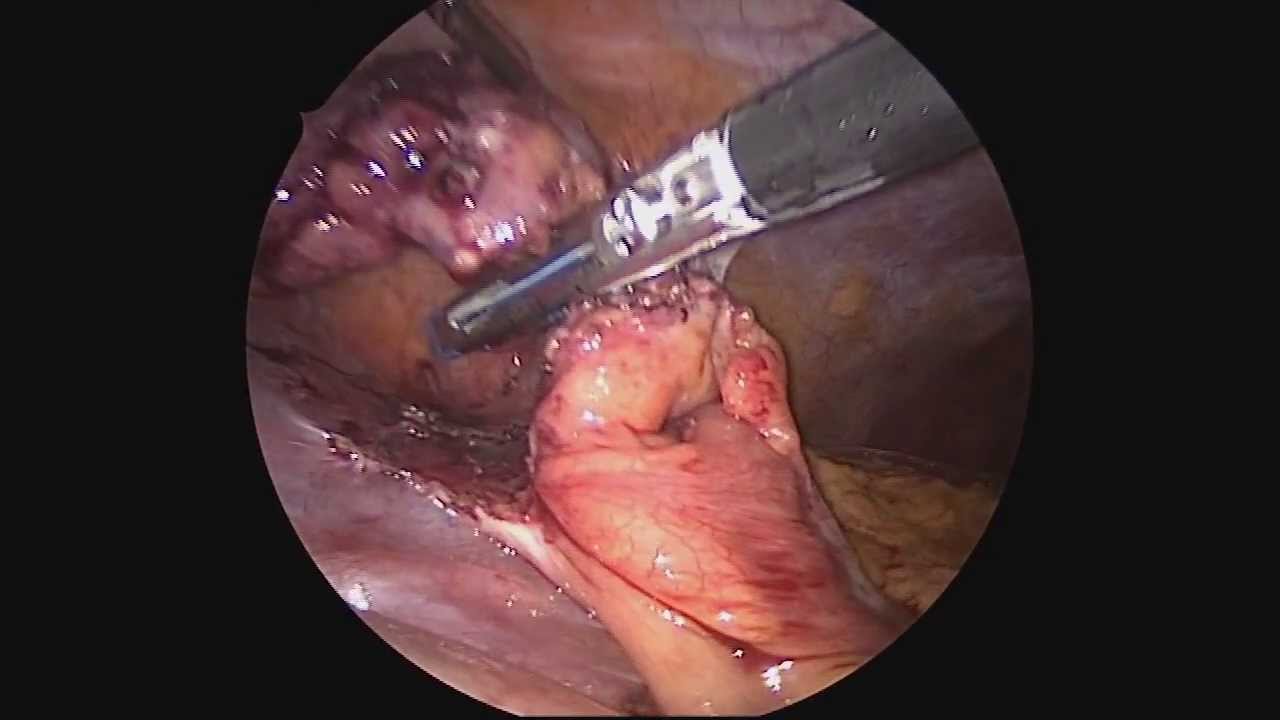
Mini-Laparoscopic Cholecystectomy with Intraoperative Cholangiogram for Symptomatic Cholelithiasis (Gallstones) - Standard
Authors: Brunt LM1, Singh R1, Yee A2
Published: September 26, 2017
AUTHOR INFORMATION
1 Department of Surgery, Washington University, St. Louis, Missouri
2 Division of Plastic and Reconstructive Surgery, Washington University, St. Louis, Missouri
DISCLOSURE
No authors have a financial interest in any of the products, devices, or drugs mentioned in this production or publication.
ABSTRACT
Minimal invasive laparoscopic cholecystectomy is the typical surgical treatment for cholelithiasis (gallstones), where patients present with a history of upper abdominal pain and episodes of biliary colic. The classic technique for minimal invasive laparoscopic cholecystectomy involves four ports: one umbilicus port, two subcostal ports, and a single epigastric port. The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) has instituted a six-step strategy to foster a universal culture of safety for cholecystectomy and minimize risk of bile duct injury. The technical steps are documented within the context of the surgical video for (1) achieving a critical view of safety for identification of the cystic duct and artery, (2) intraoperative time-out prior to management of the ductal structures, (3) recognizing the zone of significant risk of injury, and (4) routine intraoperative cholangiography for imaging of the biliary tree. In this case, the patient presented with symptomatic biliary colic due to a gallstone seen on the ultrasound in the gallbladder. The patient was managed a mini-laparoscopic cholecystectomy using 3mm ports for the epigastric and subcostal port sites with intraoperative fluoroscopic cholangiogram. Specifically, the senior author encountered a tight cystic duct preventing the insertion of the cholangiocatheter and the surgical video describes how the author managed the cystic duct for achieving a cholangiogram, in addition to the entire technical details of laparoscopic cholecystectomy.
