- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Human Circulatory System and heart video

The Lansinoh Latch Assist has been designed to extend inverted nipples - watch this video to see how.?

A thyroid biopsy is a procedure in which a small sample of tissue is removed from the thyroid gland and looked at under a microscope for cancer, infection, or other thyroid problems. The thyroid gland is found in front of the windpipe (trachea), just below the voice box (larynx). A sample of thyroid tissue can be taken by: Fine-needle biopsy. Your doctor puts a thin needle through the skin and into the thyroid gland. Many thyroid specialists like to use a needle biopsy method rather than surgery. Open biopsy. Your doctor makes a cut (incision) through the skin to see the thyroid gland. This method is done when other tests have not found the cause of your symptoms. Core needle biopsy. Your doctor inserts a needle with a special tip and removes a sample of tissue about the size of a grain of rice.
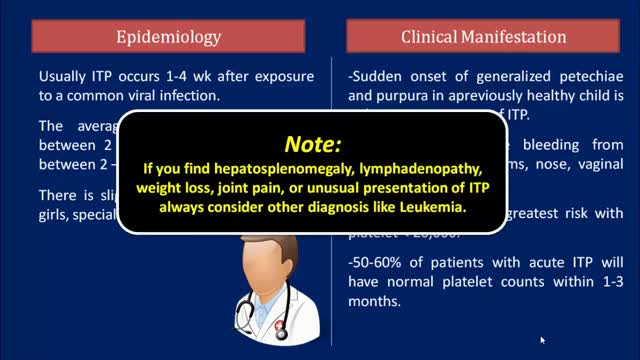
Idiopathic thrombocytopenic purpura (ITP) is a disorder that can lead to easy or excessive bruising and bleeding. The bleeding results from unusually low levels of platelets — the cells that help blood clot. Idiopathic thrombocytopenic purpura, which is also called immune thrombocytopenia, affects children and adults. Children often develop ITP after a viral infection and usually recover fully without treatment. In adults, the disorder is often long term. If you don't have signs of bleeding and your platelet count isn't too low, you may not need any treatment. In rare cases, the number of platelets may be so low that dangerous internal bleeding occurs. Treatment options are available.

First described by Aubaniac in 1952, central venous catheterization, or central line placement, is a time-honored and tested technique of quickly accessing the major venous system. Benefits over peripheral access include greater longevity without infection, line security in situ, avoidance of phlebitis, larger lumens, multiple lumens for rapid administration of combinations of drugs, a route for nutritional support, fluid administration, and central venous pressure (CVP) monitoring. Central vein catheterization is also referred to as central line placement. Overall complication rates are as high as 15%, [1, 2, 3, 4] with mechanical complications reported in 5-19% of patients, [5, 6, 7] infectious complications in 5-26%, [1, 2, 4] and thrombotic complications in 2-26%. [1, 8] These complications are all potentially life-threatening and invariably consume significant resources to treat. Placement of a central vein catheter is a common procedure, and house staff require substantial training and supervision to become facile with this technique. A physician should have a thorough foreknowledge of the procedure and its complications before placing a central vein catheter. The supraclavicular approach was first put into clinical practice in 1965 and is an underused method for gaining central access. It offers several advantages over the infraclavicular approach to the subclavian vein. At the insertion site, the subclavian vein is closer to the skin, and the right-side approach offers a straighter path into the subclavian vein. In addition, this site is often more accessible during cardiopulmonary resuscitation (CPR) and during active surgical cases. Finally, in patients who are obese, this anatomic area is less distorted.

Folic acid, which is also called folate, is a B vitamin. The best food sources of folic acid are fortified cereals. Folic acid plays an important role in the production of red blood cells and helps your baby's neural tube develop into her brain and spinal cord.

Use warm water and sea salt. Soak the wart for 10 to 15 minutes in warm salt water to moisten the skin. Scrape the dead skin layers off the wart using a nail file, pumice stone or mild sandpaper. You could also use your fingers, but wash them thoroughly before and after, as warts can easily spread.
Tension pneumothorax describes the progressive accumulation of air in the pleural cavity (normally a potential space) through a defect in the visceral pleura. This leads to positive pressure being maintained and increasing throughout the respiratory cycle causing vessels within the mediastinum to be compressed with catastrophic consequences if left untreated. Clinical signs include hypoxia, hypotension, tachycardia, reduced breath sounds and hyper resonance ipsilaterally, with tracheal deviation (away from the affected side) and distended neck veins being late clinical signs.
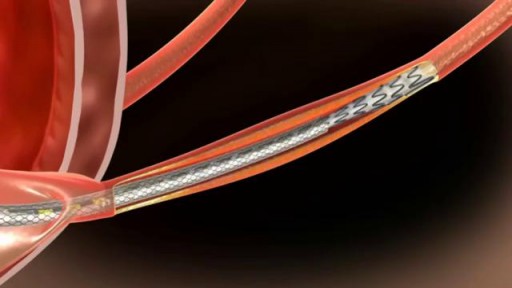
he Allium Ureteral Stents are intended for temporary long or short-term use in malignant or benign chronic Ureteral Stenosis. Allium Ureteral Stents are mounted on a ready to use 8 or 10Fr delivery system. By using the appropriate delivery system their deployment procedure can be performed either retrogradely or percutaneously. Indicated for all chronic ureteral stricturesLarge caliber for intra-lumenal flowLong dwelling timeAntegrade or retrograde insertionEasy insertion and stent positioningExcellent patient comfortNo tissue in-growthAnti-reflux designEasy removal of the device

Treatment may include: Rest. Ice or heat. Nonsteroidal anti-inflammatory medications. Strengthening exercises. Ultrasound therapy. Corticosteroid injection. Surgery (for severe injuries)

Meet Christian, an incredible man born with no arms or legs who lives life to the fullest

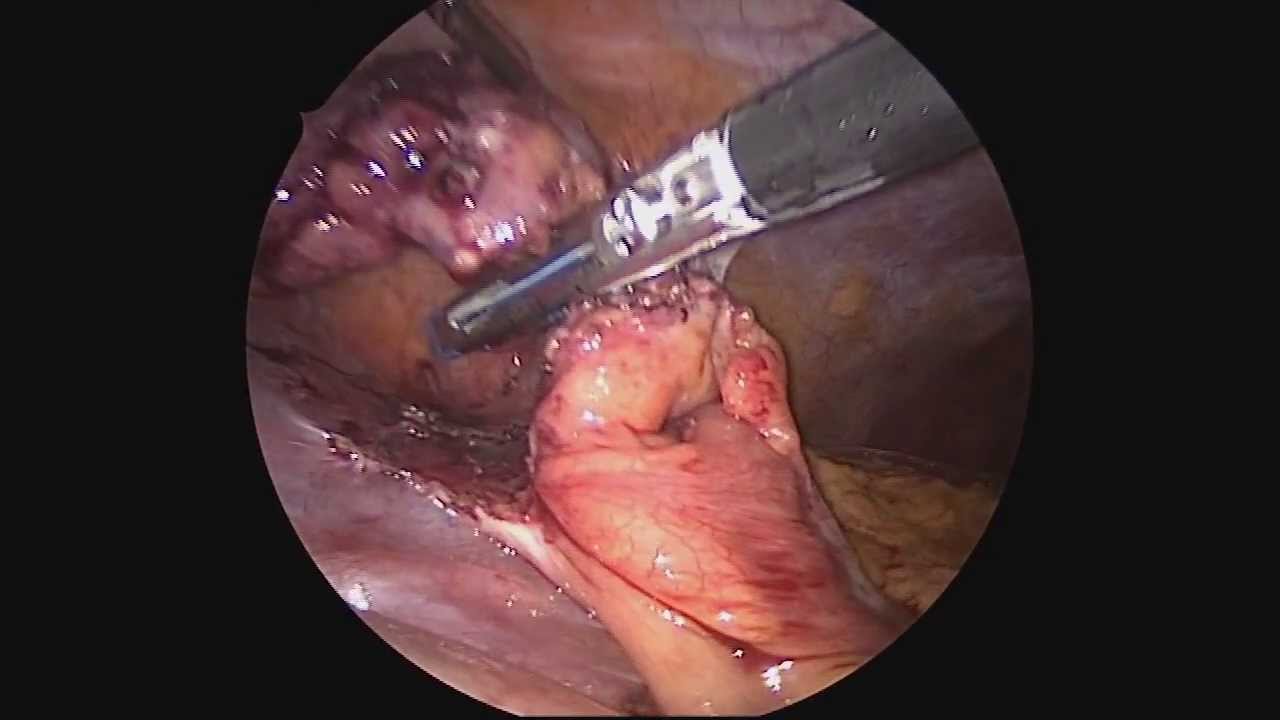
It used to be when a woman needed a hysterectomy she could expect full abdominal surgery with a long recovery time. Dr. Melissa Lee uses less invasive methods that can cut the patients downtime in half.
"We were trained in more laparoscopic and minimally invasive cases so of course that's what I'm more comfortable with doing right now."
She sees a new generation of patients opting for laparoscopic surgery.
"Laparoscopy is the use of small cameras with small incisions and instruments that are guided by the hand, and you're able to see directly into the abdomen without actually fully opening the abdomen," says Dr. Lee, an obstetrician-gynecologist with Lee Memorial Health System.
Nowadays, even a large mass or uterus can be removed using the slender tools.
"There are multiple different laparoscopic instruments that you can use. Whether they're blunt dissections or just dissectors that hold and retract back or actual scissors or cutting instruments, there are multiple different options," says Dr. Lee.
While a standard abdominal hysterectomy requires a four to eight inch incision, the laparoscope needs only a quarter to half inch. It's enough to make a big difference in terms of recovery.
"They're able to get up and move around faster. They're able to recover faster, their pain level and their need for pain medicine is much lower," says Dr. Lee.
The laparoscopic procedure also cuts down on scarring and more importantly, shortens the hospital stay. The trend now is home within 24 hours.
"Where the patient is done early in the morning, they're doing well they're tolerating oral intake they're able to getup and move around. And those patients a lot of times will feel comfortable to go home that same nigh after a major surgery," says Dr. Lee.
New studies show women who've had a laparoscopic hysterectomy viewed their quality of life as better than those who had an open abdominal procedure, making this a good option for the right patient.
View More Health Matters video segments at leememorial.org/healthmatters/
Lee Memorial Health System in Fort Myers, FL is the largest network of medical care facilities in Southwest Florida and is highly respected for its expertise, innovation and quality of care. For nearly a century, we've been providing our community with everything from primary care treatment to highly specialized care services and robotic assisted surgeries.
Visit leememorial.org
Dr. Celia Divino, Chief, Division of General Surgery at The Mount Sinai Hospital, performs a laparoscopic appendectomy. Visit the Division of General Surgery at http://bit.ly/18z944M. Click here to learn more about Dr. Celia Divino http://bit.ly/12RF0ee

Spontaneous pneumothorax is a life-threatening condition in patients with severe underlying lung disease; thus, tube thoracostomy is the procedure of choice in SSP. Pleurodesis decreases the risk of recurrence, as does thoracotomy or video-assisted thoracoscopic surgery (VATS) to excise the bullae
How do you know if you have pneumonia? They may include: Cough. You will likely cough up mucus (sputum) from your lungs. ... Fever. Fast breathing and feeling short of breath. Shaking and "teeth-chattering" chills. Chest pain that often feels worse when you cough or breathe in. Fast heartbeat. Feeling very tired or very weak. Nausea and vomiting.

Huge Pimple Draining

The video is about the evolution of the anatomic UCLA laparoscopic technique over 1325 cases and demonstrates the key steps of our operation to improve patient safety and outcomes.
Learn more at http://urology.ucla.edu

The baby suffered from ectopia cordis, a rare condition where a baby's heart is located either partially or totally outside the chest. Only 8 out of 1 million babies are born with the condition, and 90 percent of those babies are either stillborn or die within the first three days of life.

A plastic surgeon in China has successfully grown an artificial ear on a man's arm in a pioneering medical procedure. The patient, surnamed Ji, lost his right ear in an accident and yearned to have it back. Doctor Guo Shuzhong from a hospital in Xi'an, China's Shaanxi Province, used Mr Ji's cartilage from his ribs to build the new ear; and he expects to transplanted the organ to the man's head in about four months. According to the Huanqiu report, Mr Ji sustained serious injuries in the right side of his face in a traffic accident about a year ago. His right ear was torn from his face. The man, whose age is not specified, has since received multiple surgical operations to restore his facial skin and his cheeks. However, he felt frustrated about losing his right ear for good. The patient told a report from China News: 'I lost one ear. I have always felt that I am not complete.' Having sought medical advice from multiple sources, Ji realised that it was impossible to restore his ear through conventional medical procedures as a substantial part of his right ear had gone missing. Upon hearing recommendations, Mr Ji went to see doctor Guo Shuzhong, who works at the First Affiliated Hospital of Xi'an Jiaotong University in the city of Xi'an. Doctor Guo, a renowned plastic surgeon, conducted China's first face transplant operation in 2006, according to China Daily.
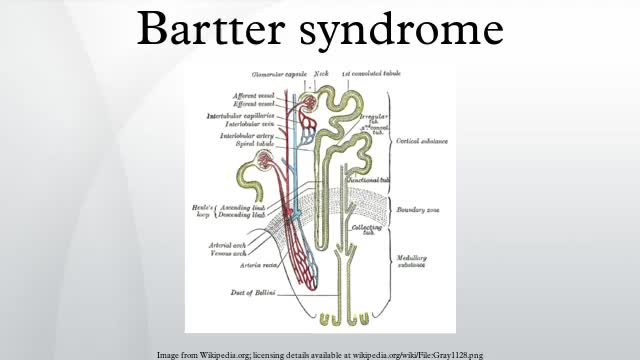
Bartter syndrome, originally described by Bartter and colleagues in 1962, [1] represents a set of closely related, autosomal recessive renal tubular disorders characterized by hypokalemia, hypochloremia, metabolic alkalosis, and hyperreninemia with normal blood pressure. The underlying renal abnormality results in excessive urinary losses of sodium, chloride, and potassium.
