- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
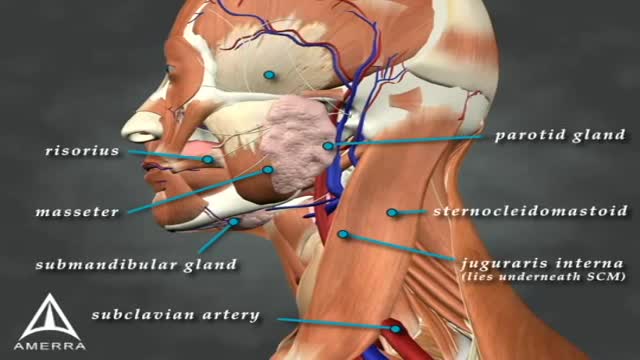
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Sialorrhea or excessive drooling is a major issue in children with cerebral palsy and adults with neurodegenerative disorders. In this review, we describe the clinical features, anatomy and physiology of sialorrhea, as well as a review of the world literature on medical treatment using Yale University’s search engine; including but not limited to Medline and Erasmus. Level of drug efficacy is defined according to the guidelines of American Academy of Neurology. Current medical management is unsatisfactory. Topical agents (scopolamine and tropicamide) and oral agents (glyccopyrolate) combined render a level B evidence (probably effective); however, this treatment is associated with troublesome side effects. Double-blind and placebo-controlled studies of botulinum toxin (BoNT) provide a level A evidence for type B (two class I studies; effective and established) and both overall and individual B level of evidence for OnabotulinumtoxinA (A/Ona) and AbobotulinumtoxinA (A/Abo); these are probably effective. For IncobotulinumtoxinA (A/Inco), the level of evidence is U (insufficient) due to lack of blinded studies. Side effects are uncommon; transient and comparable between the two types of toxin. A clinical note at the end of this review comments on fine clinical points. Administration of BoNTs into salivary glands is currently the most effective way of treating sialorrhea.
Learn the SIRS Criteria and how to calculate it. Greater than or equal to 2 or more of the following: Temperature Fever of greater than 38°C (100.4°F) or Less than 36°C (96.8°F) Heart Rate Greater than 90 beats per minute Respiratory Rate Greater than 20 breaths per minute or PaCO2 of less than 32mm Hg White Blood Cell Count Greater than 12,000cells/mm³ or Less than 4,000cells/mm³ or Greater than 10% Bands

Ocular Movement Examination
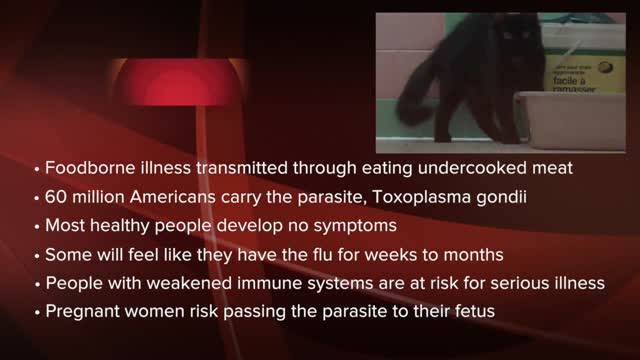
Toxoplasmosis (tok-so-plaz-MOE-sis) is a disease that results from infection with the Toxoplasma gondii parasite, one of the world's most common parasites. Toxoplasmosis may cause flu-like symptoms in some people, but most people affected never develop signs and symptoms. For infants born to infected mothers and for people with weakened immune systems, toxoplasmosis can cause extremely serious complications. If you're generally healthy, you probably won't need any treatment for toxoplasmosis. If you are pregnant or have lowered immunity, certain medications can help reduce the infection's severity. The best approach, though, is prevention.

Description: Use warm water and sea salt. Soak the wart for 10 to 15 minutes in warm salt water to moisten the skin. Scrape the dead skin layers off the wart using a nail file, pumice stone or mild sandpaper. You could also use your fingers, but wash them thoroughly before and after, as warts can easily spread.
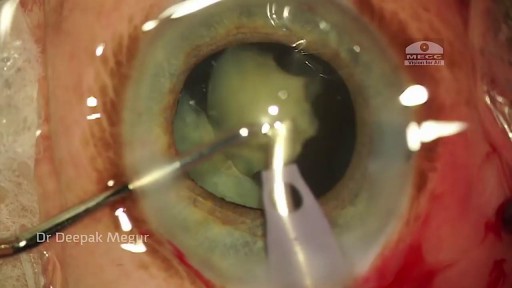
Phacolytic glaucoma usually is associated with a mature or hypermature cataract and typically occurs in elderly patients. Today, phacolytic glaucoma is rare in the United States, found primarily in areas where access to care is poor. Will the increase in the number of under- and uninsured patients lead to an increase in this condition? Evaluation and Diagnosis Signs and symptoms. Patients typically report acute-onset pain, decreased vision, tearing and photophobia. Examination will reveal injection, corneal edema, elevated IOP, anterior chamber reaction with or without pseudohypopyon, particles on the lens capsule and anterior capsule wrinkling. Patient history. The duration of symptoms should be elicited; a delayed presentation of more than five days since onset can result in glaucomatous disc damage and poorer prognosis.¹ The ocular history may reveal that the patient decided against removal of an advanced cataract. Prior intraocular surgery or trauma may have left residual lens material that could cause phacoanaphylactic glaucoma or exacerbate infectious endophthalmitis. Visual acuity and visual potential should be assessed. Exam essentials. A complete ophthalmologic examination should be done. The eye should be inflamed, and the cornea may be edematous due to the high IOP. The anterior chamber will demonstrate massive inflammation and/ or pseudohypopyon. Gonioscopy is essential; it will help rule out angle closure due to phacomorphic glaucoma or neovascularization of the angle. Assess ment of the posterior pole should be performed to rule out vitreous hemorrhage (which can result in ghost-cell glaucoma) or vitritis (which may be associated with infectious endophthalmitis or panuveitis). If the view to the fundus is obstructed, B-scan ultrasonography also should be performed. Differential diagnosis. The differential diagnosis includes infectious endophthalmitis, phacoanaphylactic glaucoma, inflammatory glaucoma, glaucoma secondary to intraocular tumor, phacomorphic glaucoma, acute-angle closure glaucoma and neovascular glaucoma. Management Medication. Medical management is used to temporarily control the glaucoma and inflammation. Initial treatment consists of hyperosmotic agents, aqueous suppressants, anti-inflammatory drugs and cycloplegics. Surgery. Definitive treatment is removal of the lens via extracapsular cataract extraction with or without an IOL. Some ophthalmologists defer placement of an IOL until after the inflammation subsides; however, there is no significant difference in final visual acuity between those patients who did receive an IOL and those who did not.¹ If the phacolytic glaucoma is of long duration (more than seven days), a combined trabeculectomy may be needed to prevent postoperative IOP spikes.² In eyes with hypermature Morgagnian cataracts, one must be especially careful, as the capsule is fragile, the zonules are weak and the view is difficult due to the white, milky cortex. Vision limited to light perception on presentation is not a contraindication to performing cataract extraction. Surgical Tips For a planned extracapsular cataract extraction with a posterior chamber IOL, fashion a superior fornix-based conjunctival flap.³ Make a partial-thickness incision along the sclerolimbal junction superiorly for 120 degrees with a No. 69 blade. Forty-five degrees away, a paracentesis should be done to decompress the eye. The anterior chamber fluid can be withdrawn for analysis, to look for macrophages and high molecular-weight proteins. Inject balanced salt solution in a cannula to wash out any residual particulate matter, then inject Healon or viscoelastic into the anterior chamber. Make an incision entering the anterior chamber at the 12 o’clock position with a keratome. A 26-gauge cystotome mounted on a syringe is then introduced through the 12 o’clock incision and used to puncture the capsular bag. The milky cortex should be aspirated as much as possible, until the nucleus is visible. Withdraw the needle through the keratome incision, then inject Healon through the 12 o’clock incision into the capsular bag. Next, enlarge the corneoscleral keratome incision with curved Westcott scissors to 120 degrees. Perform a partial V-shaped capsulotomy; this can be done either with the cystotome or with an angled Vannas scissors. Place viscoelastic under the nucleus to float the nucleus and sever any adhesions between the nucleus and the capsule. The nuclear portion of the lens can then be removed with an irrigating vectis (lens loop) with or without gentle pressure at the inferior limbus (6 o’clock). Irrigate and aspirate the residual cortex with the Simcoe cannula. Inspect the capsular bag; if it is intact, place a posterior chamber IOL into the bag. Close the incision with several interrupted 10-0 monofilament nylon sutures and reattach the conjunctival flap. Potential Sequelae and Prognosis Postoperatively, the patient should be managed with topical steroids and/or aqueous suppressants and hyperosmotics if necessary. Vitreous opacification behind the posterior capsule occurs in a small percentage of eyes. These vitreous opacities are typically absorbed by one to two weeks postoperatively. IOP usually is controlled without antiglaucoma medications after the cataract removal. A detailed glaucoma evaluation (including repeat gonioscopy to assess for peripheral anterior synechiae, visual field and optic nerve status) should be done to assess the extent of glaucomatous damage. The prognosis is dependent on the duration of elevated IOP, PAS and optic nerve damage. In one study, patients who were older than 60 and whose glaucoma was present for more than five days did significantly worse than a comparison group of younger individuals with shorter disease duration.

Podalic version is an obstetric procedure wherein the fetus is turned within the womb such that one or both feet present through the cervix during childbirth. It is used most often in cases where the fetus lies transversely or in another abnormal position in the womb.

Preventing Hemodialysis Catheters Problems
USMLE Step 2 CS - Common Tips This is just preview video. To get full access please visit our website : www.usmletutoring.com

Device that keeps a donor heart beating
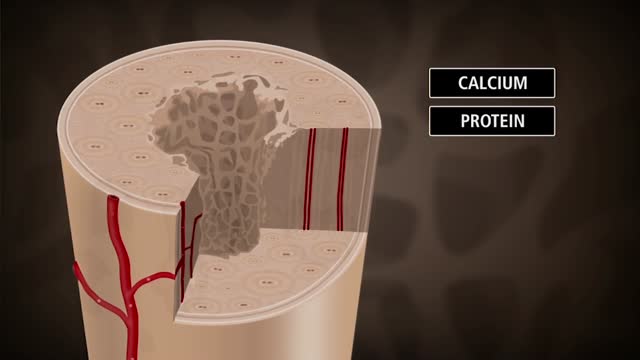
Bone is not a static part of the body — it's constantly being resorbed (broken down) and formed throughout your life. Your entire skeleton is replaced about every decade, according to the NIH. During your childhood and teenage years, bone formation occurs more quickly than bone resorption, resulting in growth. You reach your maximum bone density and strength around age 30, after which bone resorption slowly overtakes bone formation. Osteoporosis develops when there's an abnormal imbalance between bone resorption and formation — that is, resorption occurs too quickly, or formation too slowly.

Hemorrhoids repair: Disposable hemorrhoidal stapler

Psoriasis: treatment options related issues
Carotid Endartrectomy, large atheroma removed completely, patient well after surgery.
Testicular sperm aspiration (TESA) is a procedure performed for men who are having sperm retrieved for in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI). It is done with local anesthesia in the operating room or office and is coordinated with their female partner's egg retrieval.
Burns Handling Thermal Electrical Chemical

Blood type (or blood group) is determined, in part, by the ABO blood group antigens present on red blood cells. A blood type (also called a blood group) is a classification of blood based on the presence or absence of inherited antigenic substances on the surface of red blood cells (RBCs).
Encephalopathy means disorder or disease of the brain. In modern usage, encephalopathy does not refer to a single disease, but rather to a syndrome of global brain dysfunction; this syndrome can have many different organic and inorganic causes.

After the nose surgery the patients are advised to keep their nose taped for 2 weeks to 2 months. During the first two weeks, the surgery tapes influence both swelling and forming. From the second week on however, the nose tapes are applied just to reduce the swelling.

http://www.landging.com/respiratory-circulatory-system-animation.html
Human body circulatory system and respiratory system, 3D MOA (Mechanism of Action) animation, designed for Beijing Natural History Museum.
