- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos


Watch that video of The World's Biggest Jigger Removal
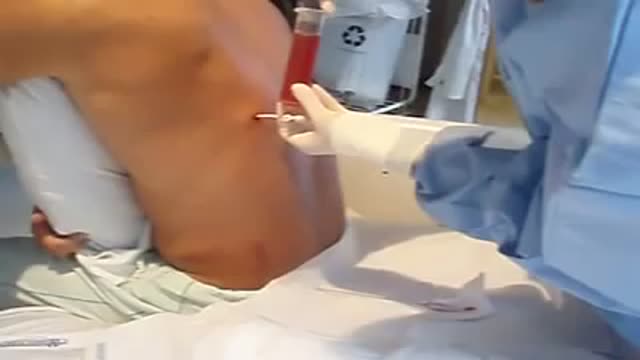
Thoracentesis is a procedure used to obtain a sample of fluid from the space around the lungs. Normally, only a thin layer of fluid is present in the area between the lungs and chest wall. However, some conditions can cause a large amount of fluid to accumulate. This collection of fluid is called a pleural effusion.

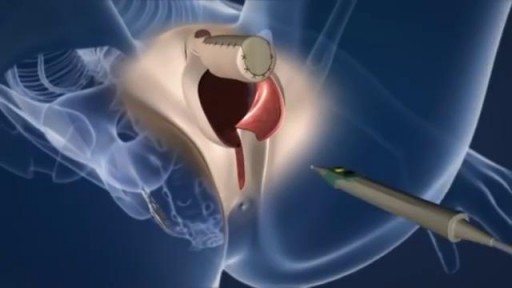
Penile Injection Therapy
When you’re trying to conceive a baby it is worth giving anything a go which you think will boost your chances. This includes considering that there may be better positions for getting pregnant. But it pays to bear in mind that the human race has been around for over 200,000 years and most of us were probably conceived without our ancestors investing too much thought into the mechanics. Science has proven that successful conception isn’t so much about sexual position as the frequency of sex between a fertile couple. Basically, if you want to fall pregnant, don’t use contraception and have frequent, active and enjoyable sex. Importantly, don’t stress too much about whether you’re doing it the right way. Women can, and do, conceive in any position. Nature has a way of making sure of that.

Your sleeping pose can have a major impact on your slumber—as well as your overall health. Poor p.m. posture could potentially cause back and neck pain, fatigue, sleep apnea, muscle cramping, impaired circulation, headaches, heartburn, tummy troubles, and even premature wrinkles

A pneumothorax occurs when some of the tiny air sacs (alveoli) in a baby's lung become overinflated and burst. This causes air to leak into the space between the lung and chest wall (pleural space). The most common cause of pneumothorax is respiratory distress syndrome. This is a condition that occurs in babies who are born too early (premature). The baby's lungs lack the slippery substance (surfactant) that helps them stay open. Therefore, the tiny air sacs are not able to expand as easily. If the baby is put on a breathing machine (mechanical ventilator), there is extra pressure on the baby's lungs, which can sometimes burst the air sacs.
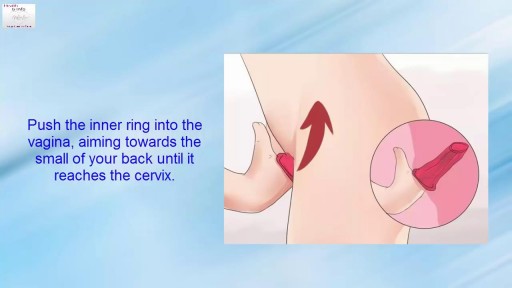
How to Use a Female Condom Step by Step

Mr Bean visits the hospital for a very peculiar reason!

If you use condoms perfectly every single time you have sex, they’re 98% effective at preventing pregnancy. But people aren’t perfect, so in real life condoms are about 85% effective — that means about 15 out of 100 people who use condoms as their only birth control method will get pregnant each year.

The OrthoIllustrated® animation for total knee replacement is an educational tool to help patients better understand the diagnosis and treatment of arthritis.
- - - - -
Why Work Arthrex https://www.arthrex.com/job-seeker
Find an Arthrex Surgeon: https://doctorfinder.orthoillustrated.com
- - - - -
Join the Community:
LinkedIn: https://www.linkedin.com/company/arthrex
Facebook: https://www.facebook.com/Arthrex
Instagram: https://www.instagram.com/arthrex_inc/
Twitter: https://twitter.com/Arthrex
TikTok: https://www.tiktok.com/@arthrex
- - - - -
Arthrex Inc., headquartered in Naples, Florida, is a global leader in orthopedic surgical device design, research, manufacturing, and medical education. Arthrex develops and releases more than 1,000 new products and procedures every year to advance minimally invasive orthopedics worldwide.
For more information, visit https://www.arthrex.com
- - - - -
OrthoPedia is an innovative educational website that was created for anyone interested in learning about orthopedics from the first-year student to the experienced orthopedic surgeon.
Visit https://www.orthopedia.com to experience the future of Medical Education.
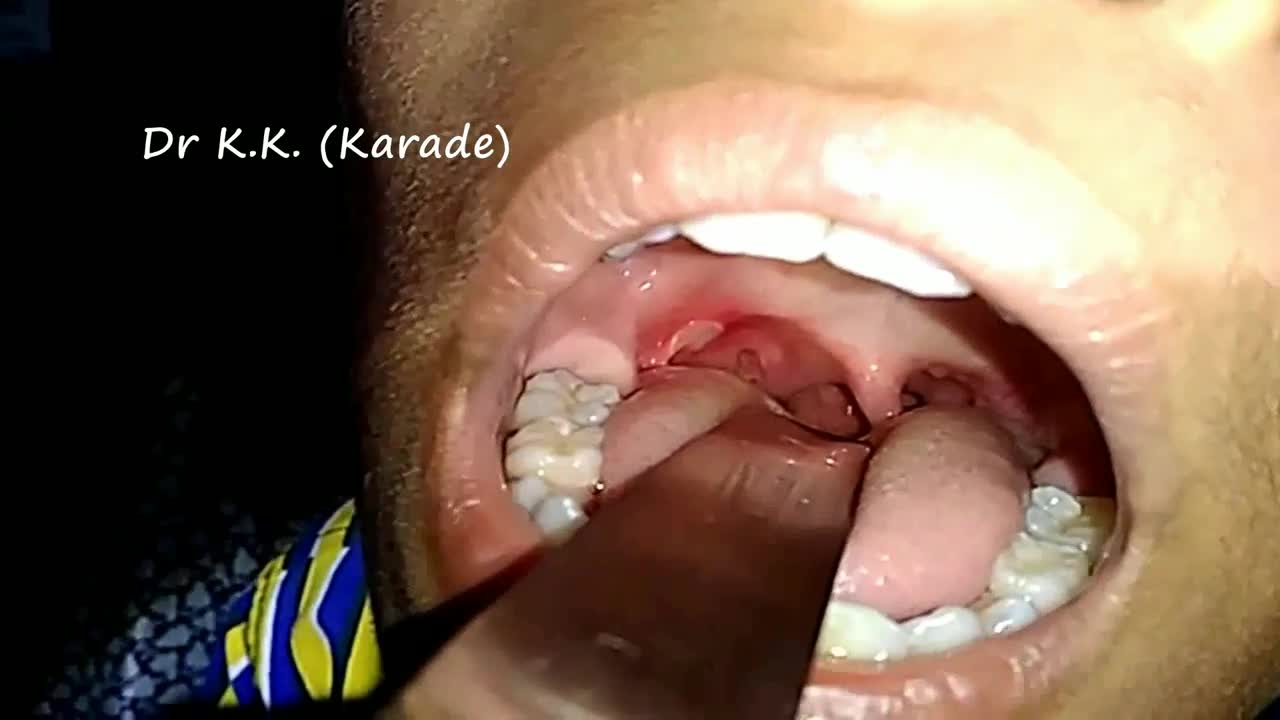
Canker sores (Aphthous ulcer) are small, painful ulcers on the inside of the mouth, tongue, lips, or throat.Canker sores are white or yellow and surrounded by a bright red area. They are not cancerous.
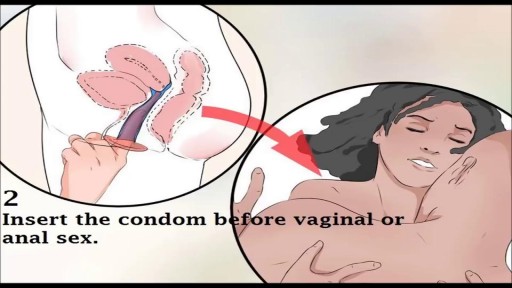
Watch that video to know How to Use Female Condom
INDICATIONS Administration of agents into the central vasculature Central circulation and intracardiac access Maintenance of venous access Hemodialysis and plasmapheresis

Sex reassignment surgery for male-to-female involves reshaping the male genitals into a form with the appearance of, and, as far as possible, the function of female genitalia. Prior to any surgeries, patients usually undergo hormone replacement therapy (HRT), and, depending on the age at which HRT begins, facial hair removal. There are associated surgeries patients may elect to, including facial feminization surgery, breast augmentation, and various other procedures.

Female IM injection

Southern Adventist University
School of Nursing
Brought to you by:
Dana Krause
Jeremy Pastor
Christina Seminario
Taken place in Florida Hospital Hall 3rd floor.

Surgical procedure of Tonsillectomy and Adenoidectomy

A Case use dòi eat organization batters prince toilet variable witness diabetic
