- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Folic acid, which is also called folate, is a B vitamin. The best food sources of folic acid are fortified cereals. Folic acid plays an important role in the production of red blood cells and helps your baby's neural tube develop into her brain and spinal cord.
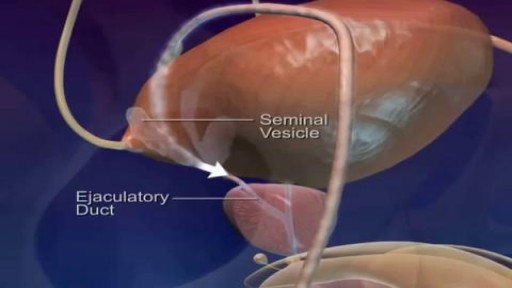
Watch that video of Pathway and Ejaculation of Sperm

Watch that video of Horrifying Things Found Living Inside Human Body

Watch that Disgusting Skin Jiggers Removing
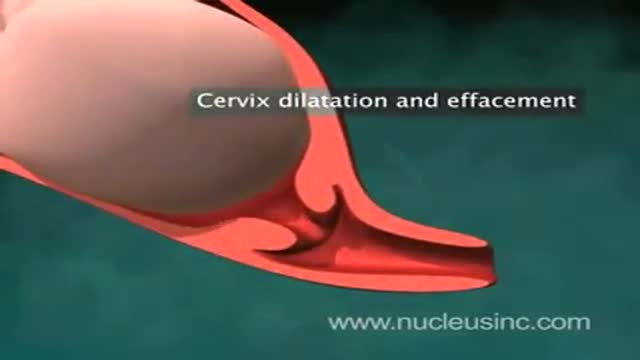
An animation showing vaginal childbirth (delivery)
Labor And Delivery During Vaginal Child Birth
At Home Weight Loss Body Wrap, Slimming Body Wraps, Inch Loss Body Wrap, It Works Body Wraps ---- http://do-body-wraps-work.plus101.com --- People are constantly one the hunt for something that will change their lives and help them lose weight. There are plenty of different options to choose from and the number of diets continues to rise. However, there is a new technique that has been gaining a lot of popularity simply because it works. If you want to really look and feel better, then you just might have to try a body wrap at home. What Can You Expect From A Body Wrap At Home? Since body wrapping is a proven therapeutic treatment, it will help detoxify your body without having to use chemicals. The nice thing about a body wrap is that it is all natural ingredients and it is by far one of the simplest ways to lose weight. You can expect to lose inches and it is a very useful addition to your current weight loss program. Why Does The Body Wrap Work? The main reason why the body wrap works so well is because you are placing all of these natural ingredients on your skin. Your skin is like your second lung because it absorbs virtually anything that you place on it. If you try the body wrap, you will instantly feel and see that this actually works. Are There Any Testimonials Saying It Works? There are plenty of testimonials saying that a body wrap at home really does help them lose inches. Though there are a few skeptics out there, the majority of people who have tried the wraps have seen results. If you are currently struggling with a crazy diet or spending half of your time in a gym, then it is time to think outside of the box and to put yourself in a wrap to finally see what your body is capable of looking like in a short period of time. Stop procrastinating! Click Here for instant access to my recipes & start losing inches, detoxifying your body, and improving your skin right away! http://do-body-wraps-work.plus101.com

A very interesting video showing how white blood cells (Neutrophil) are chasing bacteria (Diplococci). It also shows how the white blood cell engulf the bacteria. This is a real video.
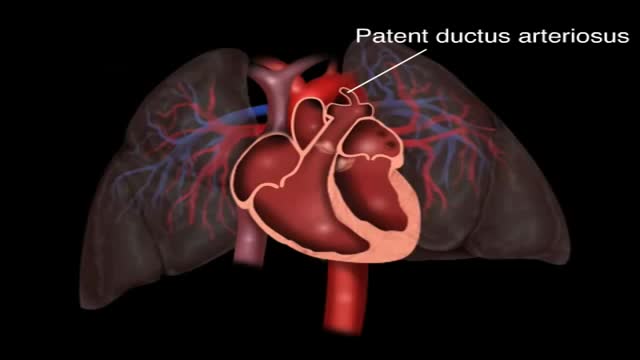
Patent ductus arteriosus (PDA) is a persistent opening between two major blood vessels leading from the heart. The opening, called the ductus arteriosus, is a normal part of a baby's circulatory system before birth that usually closes shortly after birth. If it remains open, however, it's called a patent ductus arteriosus.

Incision and Drainage of a Huge Gluteal Abscess

She is a twenty years young female presented with large cystic swelling in anterior aspect of neck. The swelling was of size 6cmx 6cm x5 cm ,tense tender, cystic just above sternal nutch.This was diagnosed as large neck abscess ./nRepeated aspiration done but the swelling reappeared. So Incision & Drainage planned under local anaesthesia./nPatient in supine position. Surgery part painted and draped. Local anaesthesia 2% xylocaine with adrenaline used for field block.After giving local anaesthesia, I used a no 11 blade for stab incision at the most prominent part of the swelling, where skin was thin and fluctuation present./nPus drained form that opening. Little dilatation of opening to be done with artery forceps or sinus forceps. Complete pus drainage to be ensured.Little finger can be introduced inside the pus cavity to ensure proper drainage of pus. The cavity I use to clean with a gauge piece. If necessary curette biopsy can be taken from the wall of the cavity.These wounds usually need daily proper dressing for faster healing.

The only sure way to prevent genital warts is to not have sex. But everyone wants sex, so here is how to have safe sex if you are living with Genital Warts.
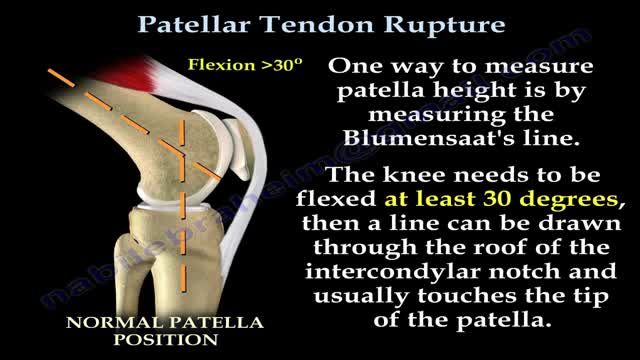
Patellar tendon rupture is a rupture of the tendon that connects the patella to the tibia. The superior portion of the patellar tendon attaches on the posterior portion of the patella, and the posterior portion of the patella tendon attaches to the tibial tubercle on the front of the tibia.

This 3D medical animation shows several methods of breast tissue biopsy procedures including:
- Needle biopsy,
- Stereotactic core biopsy
- Ultrasound-guided core biopsy - - Surgical biopsy
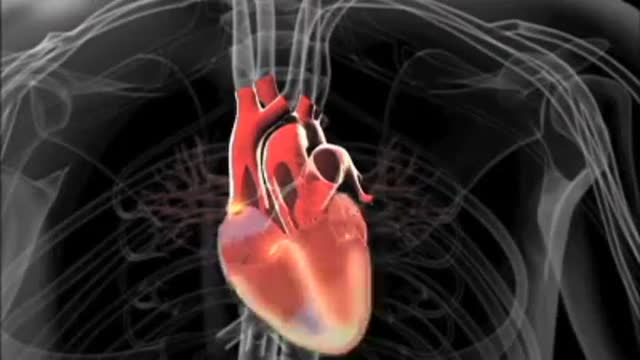
Jane Seymour sheds light on atrial fibrillation and AF-related stokes.

Ganglion cysts are noncancerous lumps that most commonly develop along the tendons or joints of your wrists or hands. They also may occur in the ankles and feet. Ganglion cysts are typically round or oval and are filled with a jellylike fluid. Small ganglion cysts can be pea-sized, while larger ones can be around an inch (2.5 centimeters) in diameter. Ganglion cysts can be painful if they press on a nearby nerve. Their location can sometimes interfere with joint movement. If your ganglion cyst is causing you problems, your doctor may suggest trying to drain the cyst with a needle. Removing the cyst surgically also is an option. But if you have no symptoms, no treatment is necessary. In many cases, the cysts go away on their own.

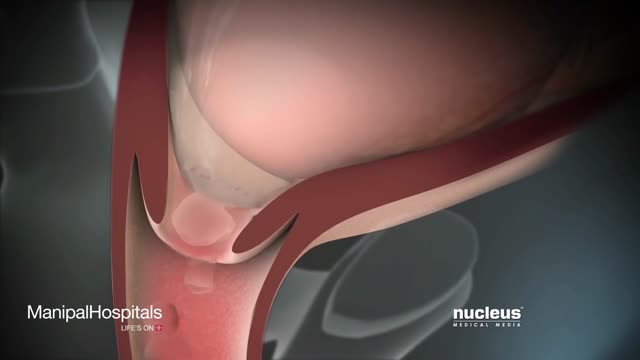
http://www.mediplus.co.uk A new and safer method of inserting a Foley catheter suprapubically. The technique allows the insertion to be carried out in an Outpatient setting, thus saving time, cost and effort. By using the Seldinger technique, the product reduces the chances of bowel or bladder perforation and resultant morbidity.
The product has been chosen by The NHS National Technology Adoption Centre to help facilitate adoption of the product

Watch that video of Closing Ejaculation Canal to Stop Sperm Surgery

A Texas baby, born with part of her heart outside her body ( Ectopia Cordis) , defies the odds and leaves hospital following a successful surgery.
Posterior Urethral Strictures Associated with Urinary Incontinence after Prostatectomy Management
