- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Click here to subscribe to Dr. Pimple Popper: https://www.youtube.com/@DrPimplePopper/
Join All Access Memberships here:
https://www.youtube.com/channe....l/UCgrsF4TYwmrV0QsXb
Click here to see my favorite POPS:
Most Popular Pops: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Blackheads: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
DPOW’s: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Steatocystomas: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Cysts: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Lipomas: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Soft Pops: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Poppin Off' Show with Dr Pimple Popper: https://youtube.com/playlist?l....ist=PLJZ_ok3xiAi_XPY
__
Connect with Dr. Pimple Popper on Social Media:
Follow Dr. Pimple Popper on Instagram: https://bit.ly/3smTOED
Follow Dr. Pimple Popper on TikTok: https://bit.ly/2MXWDM9
Follow Dr. Pimple Popper on Facebook: https://bit.ly/3oU3Rz7
Follow Dr. Pimple Popper on Twitter: https://bit.ly/2MXWDM9
Follow Dr. Sandra Lee on Instagram: https://bit.ly/2LscBO8
Subscribe to SLMD YouTube to never miss a skincare video:
https://www.youtube.com/@SLMDskincare
More ways to connect with me:
Download the Dr. Pimple Popper All Access App:
https://apps.apple.com/us/app/....dr-pimple-popper/id1
Click here to begin free trial of All-Access: https://allaccess.drpimplepopper.com/
Welcome to the world of Dr. Pimple Popper, the one and only Sandra Lee, MD! As a board certified dermatologist, skin cancer surgeon, and cosmetic surgeon, I am a highly sought-after expert in the field of dermatology.
On this channel, you'll find a treasure trove of videos that offer a window into my world.
Hopefully you'll learn about various skin conditions, hair and nail issues, and cutting-edge cosmetic surgery techniques. Whether you're struggling with blackheads, acne, cysts, warts, or looking for Botox, fillers, or liposuction, you'll find helpful advice and information here.
But this channel isn't just about skin care - it's about the amazing people I encounter every day. You'll get to know some of my incredible patients and their stories, and maybe even fall in love with dermatology just as much as I have!
Disclaimer: This video may contain dermatologic surgical and/or procedural content. The content seen in this video is provided only for medical education purposes and is not intended to be a substitute for professional medical advice, diagnosis, or treatment.
#DrPimplePopper #DrSandraLee #Dermatology #SLMD #Skincare
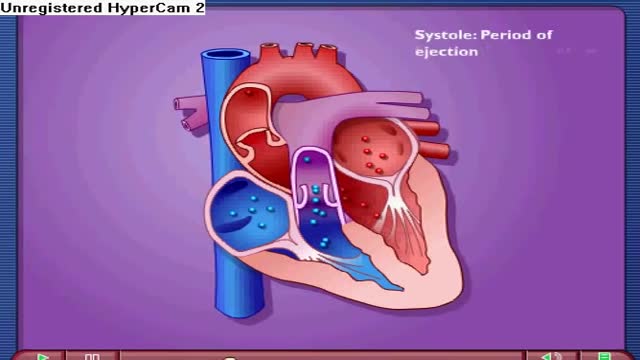
Near the end of diastole, the ventricles nearly fill with blood, and then the atria contract, adding even more volume to the ventricles. The volume of blood in the ventricles at the end of diastole is referred to as the end-diastolic volume. The other phase of the cardiac cycle is called systole.

A pneumothorax occurs when some of the tiny air sacs (alveoli) in a baby's lung become overinflated and burst. This causes air to leak into the space between the lung and chest wall (pleural space). The most common cause of pneumothorax is respiratory distress syndrome. This is a condition that occurs in babies who are born too early (premature). The baby's lungs lack the slippery substance (surfactant) that helps them stay open. Therefore, the tiny air sacs are not able to expand as easily. If the baby is put on a breathing machine (mechanical ventilator), there is extra pressure on the baby's lungs, which can sometimes burst the air sacs.

In breech position, the baby's bottom is down. There are a few types of breech: Complete breech means the baby is bottom-first, with knees bent. Frank breech means the baby's legs are stretched up, with feet near the head. Footling breech means one leg is lowered over the mother's cervix. You are more likely to have a breech baby if you: Go into early labor Have an abnormally shaped uterus, fibroids, or too much amniotic fluid Have more than one baby in your womb Have placenta previa (when the placenta is on the lower part of the uterine wall, blocking the cervix)

Examination of Peripheral Vascular System - Clinical Skills OSCE Revision - Dr Gill
In this video, we demonstrate the peripheral vascular examination - a less common examination, but still vitally important, particularly amongst the older population
Starting with the examination of the hands looking for clinical signs of vascular compromise, we then check the pulses of the major arteries of the upper body - the radial, brachial and carotid arteries, before moving down to assess for an abdominal aortic aneurysm.
At this point, I feel it's a practical step to check the femoral pulses before doing the overview of the legs.
After visually assessing we must examine the major vascular areas of leg.- namely the popliteal pulses, before wrapping up around the ankle with the posterior tibial and dorsalis pedis pulses
For completeness, the cardiovascular examination is demonstrated here
https://www.youtube.com/watch?v=ECs9O5zl6XQ&t=2s
#PeripheralVascular #ClinicalSkills #DrGill

This surgical procedure helps children defeat bone cancer.

new study about the size of penis

Heart Surgery | 8 Years Old Girl Open Heart Surgery Repair
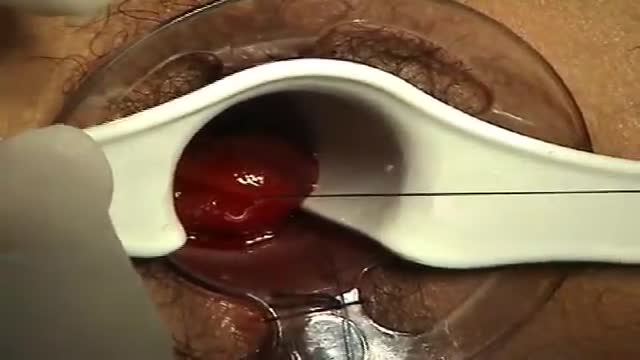
A surgeon begins the PPH stapled hemorrhoidectomy by inserting a circular anal dilator and obturator into the anal canal and then securing the dilator in place with four sutures. The surgeon then inserts a PPH anoscope into the obturator. Next, he places a circumferential purse-string suture of 2-0 Monocryl on a UR-6 needle 4 cm proximal to the dentate line. The surgeon opens a PPH stapler and places its anvil across the purse string. The stapler is then closed and fired; it is held closed for two minutes to improve hemostasis. Prior to firing the stapler in a female patient, the surgeon places a gloved finger in the vagina to ensure the vaginal mucosa and rectal-vaginal septum are not trapped within the jaws of the closed stapler. The surgeon then opens and removes the stapler.

What is inside A Cyst? Watch it now

Tongue and lip-tie are common causes of nipple pain, uneven breast drainage, slow weight gain and low milk supply. Many physicians do not properly assess for tongue or lip-tie or recognize their impact on the breastfeeding relationship, leaving babies vulnerable to early weaning. Ultrasound studies have shown that the tongue movements used by tongue-tied babies are qualitatively different from those used by by babies who are not tongue-tied. These movements are not as effective at removing milk from the breast and can cause significant pain and nipple damage. In these studies, tongue-tied babies also did not draw the nipple as deeply into the mouth as babies who were not tongue-tied.
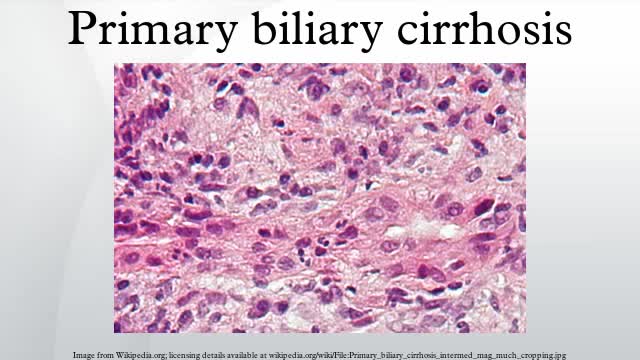
Primary biliary cirrhosis, sometimes called PBC, is a disease in which the bile ducts in your liver are slowly destroyed. Bile, a fluid produced in your liver, plays a role in digesting food and helps rid your body of worn-out red blood cells, cholesterol and toxins. When bile ducts are damaged, as in primary biliary cirrhosis, harmful substances can build up in your liver and sometimes lead to irreversible scarring of liver tissue (cirrhosis). Primary biliary cirrhosis is considered an autoimmune disease, in which the body turns against its own cells. Researchers think it is triggered by a combination of genetic and environmental factors. Primary biliary cirrhosis usually develops slowly and medication can slow its progression, especially if treatment begins early.

By 5 weeks' gestational age, the wolffian (ie, mesonephric) and the müllerian (ie, paramesonephric) ducts have formed from intermediate mesoderm. In the absence of testosterone and müllerian inhibitory substance, the mesonephric ducts regress and the paramesonephric ducts continue to form the female reproductive structures with fusion of the distal portions of the paramesonephric ducts to give rise to the uterine fundus, the cervix, and the upper vagina. These developmental changes are genetically controlled in large part by a series of complex transcriptional signaling pathways including Wnt signaling, Hox genes, and many others. In a female fetus, the wolffian duct disappears except for nonfunctional vestiges. The müllerian duct is lined by a columnar epithelium. This includes the entire cervix and upper vagina to the vaginal plate (ie, sinovaginal bulb). Through a process of squamous metaplasia, the vagina and a variable portion of the ectocervix become covered with squamous epithelium. This process is complete by the fifth month of pregnancy.
Testicle pain (testicular pain) is pain that occurs in or around one or both testicles. Sometimes testicle pain actually originates from somewhere else in the groin or abdomen, and is felt in one or both testicles (referred pain).

female condom

Compromise of the blood supply from microvascular disease, often in association with lack of sensation because of neuropathy, predisposes persons with diabetes mellitus to foot infections. These infections span the spectrum from simple, superficial cellulitis to chronic osteomyelitis. Diabetic foot infections typically take one of the following forms: Cellulitis Deep-skin and soft-tissue infections Acute osteomyelitis Chronic osteomyelitis Cellulitis Tender, erythematous, nonraised skin lesions are present, sometimes with lymphangitis Lymphangitis suggests group A streptococcal infection Bullae are typical of Staphylococcus aureus infection, but occasionally occur with group A streptococci

Infection leg gets cleaning inside
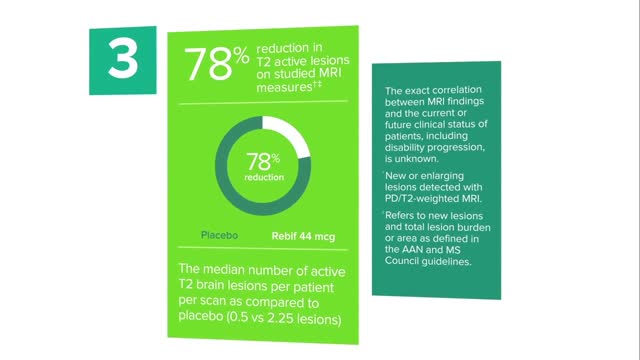
Doctors have many options to choose from, including interferon (Avonex, Betaseron, Extavia, and Rebif ), glatiramer acetate (Copaxone), mitoxantrone (Novantrone), teriflunomide (Aubagio), fingolimod (Gilenya), dimethyl fumarate (Tecfidera), and natalizumab (Tysabri).

Initial symptoms may include: Pain or discomfort in the upper tummy (abdomen), especially after eating. Indigestion. (Note: most people who have indigestion do not have stomach cancer.) Feeling sick, and being off food. ... Weight loss and/or loss of appetite. You may pass blood out with your stools (faeces).

Panic attack from Injection:'(
