- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

A Video from New England Journal of Medicine showing how to do nasogastric intubation

DMC Wound Care Specialist Doctor Bob Wilson uses the Hyperbaric Oxygen Therapy Chamber to supercharge the body's healing process from wounds, burns and infections. This new therapy works miracles on a young patient threatened with paralysis, and gets her back on the dance floor. ~ Detroit Medical Center

Open Inguinal Hernia Repair Surgery - German Narration

"Targeted" radiation therapy goes right to the problem, not throughout your system. Moreover, discomfort is minimal. ~ Detroit Medical Center

Ulnar Gutter Cast
Gunshot Wound to the Abdomen: Laparoscopic Exploration and Repair of Small Bowel Injury.

A revision knee replacement operation is shown in four parts. In this first part, an account of the patient is given on why he wanted a revision. This patient was dissatisfied with the range of movement that he got after a primary TKR. The first part shows the exposure and removal of the old implants. From www.kneeindia.com

Forehead Flap Nasal Reconstruction

Dr. David L. Sneed discusses the Austin Threadlift procedure, commonly referred to as the non-surgical facelift. This minimally-invasive skin rejuvenation procedure uses non-absorbable sutures to gently lift and tighten sagging, facial tissue and drooping skin, while at the same time stimulating further collagen growth over time. If you would like to find out more about the Silhouette Suture ThreadLift procedure offered in Austin, TX, please visit http://www.amedspa.com/silhouette-threadlift.php
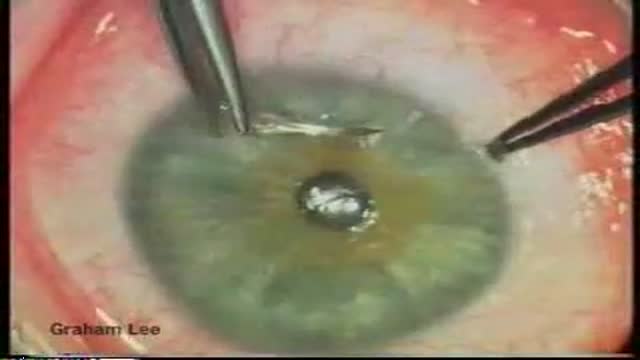
Trabeculectomy with mitomycin-C for complex glaucoma. video

This video demonstrates how to treat venereal warts or condyloma using a cryosurgery technique.

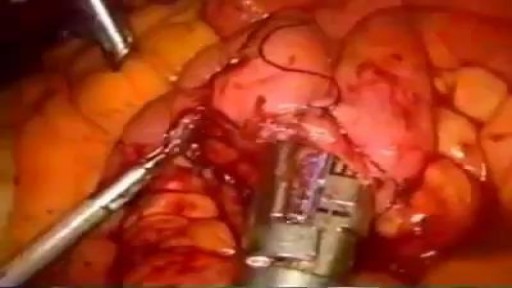
The device has as great advantage that the accessibility increases in the hand, it maximizes the surgical area free of obstacles, it increases its functional versatility, for the material with the one that this made a maximum of durability is guaranteed, so that it can be sterilized in any team and it facilitates that the thumb is supported in relaxation state.
The considerable reduction of the surgical time of each intervention is inside the advantages that it provides this valuable instrument, also facilitating that they are executed with more security. For the stability that provide, it can also be used in bony fabrics of the hand. The instrument is both handle, of very easy use and great comfort in its handling. The standardization of most of its pieces makes it very simple. The solutions that are offered in this device for the subjection of the fingers and other parts of the hand are a novelty, but they also have the advantage that it commits very little surgical area and it guarantees a maximum of subjection staying the totally stable hand facilitating in great measure the surgeon's work. These pieces adapt to any diameter of fingers.
Watch that video to know What Does Happen To Your Body When You Drown?
Hysterectomy done laparoscopically is a relative new approach to the classical hysterectomy procedure, the advantages are better anatomic views, less bleeding, less surgical time and less recovery time

laparoscopic anterior resection

Volar Slab Cast Application
A video produced by the Society of Interventional Radiology discussing the solutions that interventional radiology has to offer.
Breast Reduction Surgery video Operation مركز افارا لجراحات التجميل الخدود تكبير الشفايف

Neonatal resuscitation skills are essential for all health care providers who are involved in the delivery of newborns. The transition from fetus to newborn requires intervention by a skilled individual or team in approximately 10% of all deliveries. This figure is concerning because 81% of all babies in the United States are born in nonteaching, nonaffiliated level I or II hospitals. In such hospitals, the volume of delivery service may not be perceived as sufficient economic justification for the continuous in-hospital presence of personnel with high-risk delivery room experience, as recommended by the American Academy of Pediatrics (AAP) and the American College of Obstetricians and Gynecologists (ACOG). [1] Perinatal asphyxia and extreme prematurity are the 2 complications of pregnancy that most frequently necessitate complex resuscitation by skilled personnel. However, only 60% of asphyxiated newborns can be predicted ante partum. The remaining newborns are not identified until the time of birth. Additionally, approximately 80% of low-birth-weight infants require resuscitation and stabilization at delivery. Nearly one half of newborn deaths (many of which involve extremely premature infants) occur during the first 24 hours after birth. Many of these early deaths also have a component of asphyxia or respiratory depression as an etiology. For the surviving infants, effective management of asphyxia in the first few minutes of life may influence long-term outcome. Even though prenatal care can identify many potential fetal difficulties ante partum, allowing maternal transfer to the referral center for care, many women who experience preterm labor are not identified prospectively and therefore are not appropriately transferred to a tertiary perinatal center. Consequently, many deliveries of extremely premature infants occur in smaller hospitals. For this reason, all personnel involved in delivery room care of the newborn should be trained adequately in all aspects of neonatal resuscitation. Additionally, equipment that is appropriately sized to resuscitate infants of all gestational ages should be available in all delivering institutions, even if the institution does not care for preterm or intensive care infants. Along with the necessary skills, the practitioner should approach any resuscitation with a good comprehension of transitional physiology and adaptation, as well as an understanding of the infant's response to resuscitation. Resuscitation involves much more than possessing an ordered list of technical skills and having a resuscitation team; it requires excellent assessment skills and a grounded understanding of physiology.
Asthma and COPD
