Últimos vidéos

Respiratory Examination video

Cardiovascular Examination video

Chest examination video

Michael Marcus, MD Pediatric Pulmonary www.DrMDK.com Maimonides Medical Center Fellowship:Children’s Hospital of Philadelphia www.DrMDK.com

Michael La Corte MD
Ped Card

Henry Anhalt DO FAAP
Ped Eddo
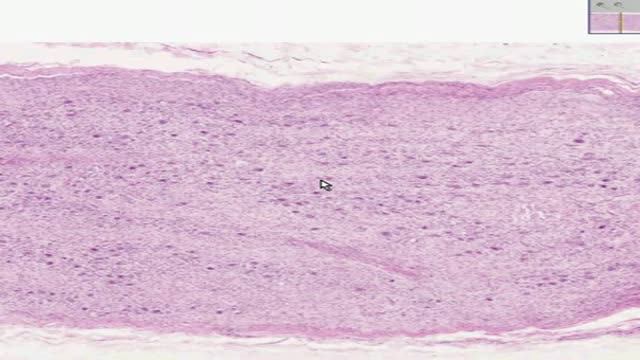
Histology of Sympathetic Ganglion
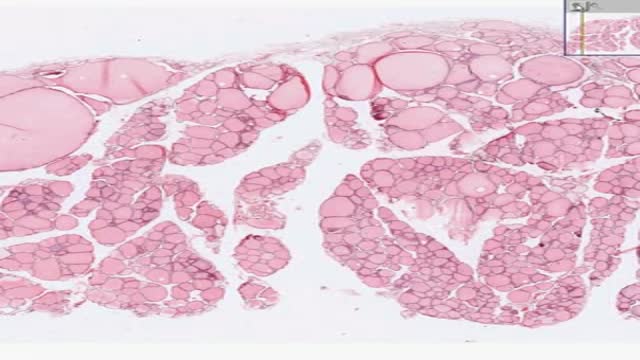
Histology of the Thyroid gland
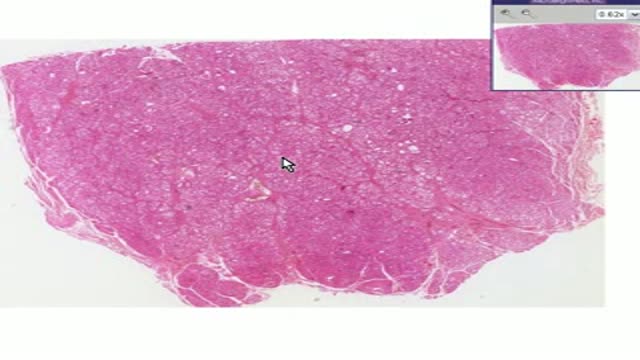
Histopathology of Graves Disease
A video showing clinical examination of the thyroid gland

Video shows a fine needle biopsy with guided ultrasound of a thyroid nodule.

thyroid gland removal is the standard procedure for thyroid cancer treatment.
Total removal of the gland is therapeutic in most cases of thyroid cancer.
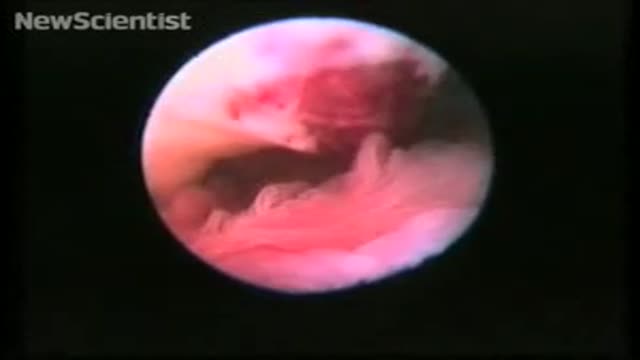
To record the sequence, Stephan Gordts and Ivo Brosens of the Leuven Institute for Fertility & Embryology in Belgium performed transvaginal laparoscopy, which involves making a small cut in the vaginal wall and observing the ovary with an endoscope.
"This allows us direct access to and observation of the tubo-ovarian structures without manipulation using forceps," says Gordts.
For the photos of ovulation, which only accidentally captured the critical moment, Jacques Donnez at the Catholic University of Louvain (UCL) in Brussels, Belgium, used gas to distend the organs for photography. However, Gordts and Brosens planned the procedure to coincide with ovulation and used saline solution to "float" the structures.
Perfect timing
Observation was timed for the day of the peak of the patient's luteal hormone cycle. Ovulation was predicted to occur on the evening of the day of the LH peak, and the endoscope introduced at 6 pm.
A small amount of saline was used to float the opening of the fallopian tube, its fimbriae (the "fingers" that sweep the egg into the tube) and the ovary itself. This gives a more natural appearance than gas, says Gordts.
In the video, the fimbriae can be seen sweeping in time with the patient's heartbeat. A mucus plug can be seen protruding from the ovary – this contains the egg.
"The ovum is not captured 'naked'," says Gordts. "There is no eruption like a volcano."
Gordts says that in clinical practice it is not easy to organise the observation of ovulation. "We were probably lucky to be successful at our first attempt," he says.

Moving Tape worm as seen by colonoscopy

A video describing the procedure of colonoscopy or flexible fibre-optic examination of the colon.

Spurting Gastric Varices (GOV 1), injected Cyanoacrylate (Histoacryl®).
Dr. Mohamed Abeid
From the " Endoscopy Atlas " :
http://www.facebook.com/group.php?gid=16900943915

Coin extraction from the upper esophagus in a child.
Dr. Mohamed Abeid
From the " Endoscopy Atlas " :
http://www.facebook.com/group.php?gid=16900943915&ref=ts

A video of appendectomy surgery performed by the laparoscope

This is the biggest known operation ever.The Whipple procedure(pancreatoduodenectomy) is the most common operation performed for pancreatic cancer and may be used to treat other cancers such as small bowel cancer. Surgeons remove the head of the pancreas, most of the duodenum (a part of the small intestine), a portion of the bile duct and sometimes a portion of the stomach. After the pancreatoduodenectomy, the surgeon reconstructs the digestive tract. At Mayo Clinic, surgeons perform more than 100 Whipple procedures annually. Patients leave the hospital in an average of 14 days.

Gluteal (Buttock) Augmentation plaatic surgery
