- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Depending on the underlying cause, some types of kidney disease can be treated. Often, though, chronic kidney disease has no cure. Treatment usually consists of measures to help control signs and symptoms, reduce complications, and slow progression of the disease. If your kidneys become severely damaged, you may need treatment for end-stage kidney disease. Treating the cause Your doctor will work to slow or control the cause of your kidney disease. Treatment options vary, depending on the cause. But kidney damage can continue to worsen even when an underlying condition, such as high blood pressure, has been controlled. Treating complications Kidney disease complications can be controlled to make you more comfortable. Treatments may include: High blood pressure medications. People with kidney disease may experience worsening high blood pressure. Your doctor may recommend medications to lower your blood pressure — commonly angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers — and to preserve kidney function. High blood pressure medications can initially decrease kidney function and change electrolyte levels, so you may need frequent blood tests to monitor your condition. Your doctor will likely also recommend a water pill (diuretic) and a low-salt diet. Medications to lower cholesterol levels. Your doctor may recommend medications called statins to lower your cholesterol. People with chronic kidney disease often experience high levels of bad cholesterol, which can increase the risk of heart disease.
Bacterial abscess of the liver is relatively rare; however, it has been described since the time of Hippocrates (400 BCE), with the first published review by Bright appearing in 1936. In 1938, Ochsner's classic review heralded surgical drainage as the definitive therapy; however, despite the more aggressive approach to treatment, the mortality remained at 60-80%.[1] The development of new radiologic techniques, the improvement in microbiologic identification, and the advancement of drainage techniques, as well as improved supportive care, have reduced mortality to 5-30%; yet, the prevalence of liver abscess has remained relatively unchanged. Untreated, this infection remains uniformly fatal. The three major forms of liver abscess, classified by etiology, are as follows: Pyogenic abscess, which is most often polymicrobial, accounts for 80% of hepatic abscess cases in the United States Amebic abscess due to Entamoeba histolytica accounts for 10% of cases [2] Fungal abscess, most often due to Candida species, accounts for fewer than 10% of cases

Pyogenic granuloma (lobular capillary hemangioma[1] ) is a relatively common benign vascular lesion of the skin and mucosa whose exact cause is unknown. Also see the Medscape Reference article Oral Pyogenic Granuloma. Pyogenic granulomas are misnamed; they are neither infectious nor granulomatous. The lesion usually occurs in children and young adults as a solitary, glistening red papule or nodule that is prone to bleeding and ulceration. Pyogenic granulomas typically evolve rapidly over a period of a few weeks, most often on the head, neck, extremities, and upper trunk. Pyogenic granuloma often arises in pregnancy (or rarely with oral contraceptive usage), particularly on the gingiva or elsewhere in the oral mucosa, and then is termed the "pregnancy tumor." Other pyogenic granuloma variants that have been well documented include the disseminated, subcutaneous, intravenous, and medication-induced (for example, retinoid, antiretroviral, and oncologic agent) subtypes. Removal of pyogenic granuloma is indicated to alleviate any bleeding, discomfort, cosmetic distress, and diagnostic uncertainty. A number of malignant tumors may clinically mimic pyogenic granuloma, making histopathologic confirmation important if the presentation is atypical. Aside from cutaneous and oral lesions, pyogenic granuloma has been reported throughout the gastrointestinal tract and upper airway, at various ocular locations, the central nervous system, the bladder, and the internal vasculature. This article discusses only cutaneous and oral involvement.

Pyogenic liver abscess Email this page to a friend Email this page to a friend Facebook Twitter Google+ Pyogenic liver abscess is a pus-filled area in the liver. Causes There are many potential causes of liver abscesses, including: Abdominal infection, such as appendicitis, diverticulitis, or a perforated bowel Infection in the blood Infection of the bile draining tubes Recent endoscopy of the bile draining tubes Trauma that damages the liver The most common bacteria that cause liver abscesses are: Escherichia coli Bacteroides Enterococcus Klebsiella pneumoniae Staphylococcus aureus Streptococcus In most cases, more than one type of bacteria is found.

The Blood Flow In Leg
People with Extremely Large Body Parts
Tobacco use is the most common preventable cause of death. About half of the people who don't quit smoking will die of smoking-related problems. Quitting smoking is important for your health. Soon after you quit, your circulation begins to improve, and your blood pressure starts to return to normal. Your sense of smell and taste return, and it's easier for you to breathe. In the long term, giving up tobacco can help you live longer. Your risk of getting cancer decreases with each year you stay smoke-free. Quitting is not easy. You may have short-term affects such as weight gain, irritability, and anxiety. Some people try several times before they succeed. There are many ways to quit smoking. Some people stop "cold turkey." Others benefit from step-by-step manuals, counseling, or medicines or products that help reduce nicotine addiction. Some people think that switching to e-cigarettes can help you quit smoking, but that has not been proven. Your health care provider can help you find the best way for you to quit.
Knee pain facts Knee pain is a common problem with many causes, from acute injuries to complications of medical conditions. Knee pain can be localized to a specific area of the knee or be diffuse throughout the knee. Knee pain is often accompanied by physical restriction. A thorough physical examination will usually establish the diagnosis of knee pain. The treatment of knee pain depends on the underlying cause. The prognosis of knee pain is usually good although it might require surgery or other interventions.

Anemia is a medical condition in which the red blood cell count or hemoglobin is less than normal. The normal level of hemoglobin is generally different in males and females. For men, a normal hemoglobin level is typically defined as a level of more than 13.5 gram/100 ml, and in women as hemoglobin of more than 12.0 gram/100 ml. These definitions may vary slightly depending on the source and the laboratory reference used. Continue Reading

Cellulitis (sel-u-LIE-tis) is a common, potentially serious bacterial skin infection. Cellulitis appears as a swollen, red area of skin that feels hot and tender. It can spread rapidly to other parts of the body. Cellulitis isn't usually spread from person to person. Skin on lower legs is most commonly affected, though cellulitis can occur anywhere on your body or face. Cellulitis might affect only your skin's surface. Or it might also affect tissues underlying your skin and can spread to your lymph nodes and bloodstream. Left untreated, the spreading infection can rapidly turn life-threatening. It's important to seek immediate medical attention if cellulitis symptoms occur.

The human heart has four main valves—two on the left and two on the right. The aortic valve is one of the main valves on the left side of the heart. It is the outflow valve for the left ventricle, which means that it is the valve between the heart and the body. The aortic valve opens when the left ventricle squeezes to pump out blood, and closes in between heart beats to keep blood from going backward into the heart.

A central venous catheter (CVC), also known as a central line, central venous line, or central venous access catheter, is a catheter placed into a large vein. Catheters can be placed in veins in the neck (internal jugular vein), chest (subclavian vein or axillary vein), groin (femoral vein), or through veins in the arms (also known as a PICC line, or peripherally inserted central catheters). It is used to administer medication or fluids that are unable to be taken by mouth or would harm a smaller peripheral vein, obtain blood tests (specifically the "central venous oxygen saturation"), and measure central venous pressure.

A lumbar puncture (also called a spinal tap) is a procedure to collect and look at the fluid (cerebrospinal fluid, or CSF) surrounding the brain and spinal cord. During a lumbar puncture, a needle is carefully inserted into the spinal canal low in the back (lumbar area). Samples of CSF are collected.

Folic acid, which is also called folate, is a B vitamin. The best food sources of folic acid are fortified cereals. Folic acid plays an important role in the production of red blood cells and helps your baby's neural tube develop into her brain and spinal cord.

Easy Exercises for Normal Delivery

An unnamed Russian scientist has introduced the concept of a device that attaches to the wall of the artery. It would first stop blood flow to the area to prevent breakaway plaque. A drill would then scrape the plaque from the artery wall. The procedure of treating plaque buildup could include bypass surgery, stent replacement and balloon angioplasty. Since the plaques are of different types and locations in the body, the inventor proposed using different types of cutting mills.
Valvular stenosis occurs when one or more heart valves are narrowed, stiffened, thickened or blocked. A variety of treatment options are available for this disorder. Learn more about the treatments on: bit.ly/2g6Mh8f
Diabetic retinopathy (die-uh-BET-ik ret-ih-NOP-uh-thee) is a diabetes complication that affects eyes. It's caused by damage to the blood vessels of the light-sensitive tissue at the back of the eye (retina). At first, diabetic retinopathy may cause no symptoms or only mild vision problems. Eventually, it can cause blindness. The condition can develop in anyone who has type 1 or type 2 diabetes. The longer you have diabetes and the less controlled your blood sugar is, the more likely you are to develop this eye complication.

Diabetic neuropathy is a type of nerve damage that can occur if you have diabetes. High blood sugar (glucose) can injure nerve fibers throughout your body, but diabetic neuropathy most often damages nerves in your legs and feet. Depending on the affected nerves, symptoms of diabetic neuropathy can range from pain and numbness in your extremities to problems with your digestive system, urinary tract, blood vessels and heart. For some people, these symptoms are mild; for others, diabetic neuropathy can be painful, disabling and even fatal. Diabetic neuropathy is a common serious complication of diabetes. Yet you can often prevent diabetic neuropathy or slow its progress with tight blood sugar control and a healthy lifestyle.
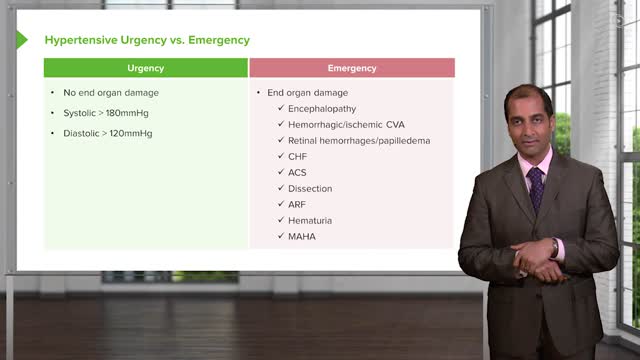
The Hypertensive urgency must be distinguished from hypertensive emergency. Urgency is defined as severely elevated blood pressure (ie, systolic >220 mm Hg or diastolic >120 mm Hg) with no evidence of target organ damage.
