- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Surgeons Open Chest of Stabbed Patient to Pull Knife Out of His Heart

Surgical drainage of dental abscess extending Into the Sub mandibular Space

Large Leg Abscess

28 years old gentleman presented with huge liver abscess in the right lobe, with repeated attempts of percutaneous aspirations in the past. He was evaluated and subjected to Laparoscopic drainage. This video depicts feasibility of laparoscopy in deep seated liver abscesses. Video created by: Dr. Juneed M. Lanker Fellow Minimal Access Surgery Apollo Hospitals Chennai.

Curious about physiotherapy or wanting to know how to properly perform an exercise? Check us out on Social Media! Facebook: https://www.facebook.com/striveptandperformance/ Instagram: https://www.instagram.com/striveptandperf/ Twitter: https://twitter.com/StrivePTandPerf Blog: http://www.strivept.ca/blog

A flail chest occurs when a segment of the thoracic cage is separated from the rest of the chest wall. This is usually defined as at least two fractures per rib (producing a free segment), in at least two ribs. A segment of the chest wall that is flail is unable to contribute to lung expansion. Large flail segments will involve a much greater proportion of the chest wall and may extend bilaterally or involve the sternum. In these cases the disruption of normal pulmonary mechanics may be large enough to require mechanical ventilation.

Paradoxical movement is an obvious sign that the portion of the chest wall is not assisting with the breathing function. Other symptoms of flail chest can include: Bruises, grazes, and/or discoloration in the chest area. Telltale markings from a seat belt.

Intrauterine insemination (IUI) is a fertility treatment that involves placing sperm inside a woman's uterus to facilitate fertilization. The goal of IUI is to increase the number of sperm that reach the fallopian tubes and subsequently increase the chance of fertilization

Massive bone defects (>8 cm) will not unite without an additional intervention. They require a predictable, durable, and efficient method to regrow bone. The Ilizarov method of tension stress, or distraction osteogenesis, first involves a low-energy osteotomy1 - 5. The bone segments are then pulled apart, most often using an external device at a specific rate and rhythm (distraction phase), after which the newly formed bone (the regenerate) requires time for consolidation. The consolidation phase is variable and usually requires a substantially greater amount of time before the external device can be removed. Our technique of tibial bone transport over an intramedullary nail using cable and pulleys combines internal and external fixation, allowing the external fixator to be removed at the end of the distraction phase. This increases the efficiency of limb reconstruction and decreases the external-fixator-associated complications.

Popping and draining a leg abscess

Popping a Big Zit on the Face
A diaphragm is a shallow, bendable cup that you put inside your vagina. It covers your cervix during sex to prevent pregnancy.


Always consult your doctor and seek help early enough to prevent complications

Skin grafting is a type of medical grafting involving the transplantation of skin. The transplanted tissue is called a skin graft. Skin grafting is often used to treat: Extensive wounding or trauma Burns Areas of extensive skin loss due to infection such as necrotizing fasciitis or purpura fulminans Specific surgeries that may require skin grafts for healing to occur – most commonly removal of skin cancers. Skin grafts are often employed after serious injuries when some of the body’s skin is damaged. Surgical removal (excision or debridement) of the damaged skin is followed by skin grafting. The grafting serves two purposes: it can reduce the course of treatment needed (and time in the hospital), and it can improve the function and appearance of the area of the body which receives the skin graft. There are two types of skin grafts, the more common type is where a thin layer is removed from a healthy part of the body (the donor section), like peeling a potato, or a full thickness skin graft, which involves pitching and cutting skin away from the donor section. A full thickness skin graft is more risky, in terms of the body accepting the skin, yet it leaves only a scar line on the donor section, similar to a Cesarean section scar. For full thickness skin grafts, the donor section will often heal much more quickly than the injury and is less painful than a partial thickness skin graft.

A burn is tissue damage that results from scalding, overexposure to the sun or other radiation, contact with flames, chemicals or electricity, or smoke inhalation. Is it a major or minor burn? Call 911 or seek immediate care for major burns, which: Are deep Cause the skin to be dry and leathery May appear charred or have patches of white, brown or black Are larger than 3 inches (about 8 centimeters) in diameter or cover the hands, feet, face, groin, buttocks or a major joint A minor burn that doesn't require emergency care may involve: Superficial redness similar to a sunburn Pain Blisters An area no larger than 3 inches (about 8 centimeters) in diameter Treating major burns Until emergency help arrives: Protect the burned person from further harm. If you can do so safely, make sure the person you're helping is not in contact with the source of the burn. For electrical burns, make sure the power source is off before you approach the burned person. Make certain that the person burned is breathing. If needed, begin rescue breathing if you know how. Remove jewelry, belts and other restrictive items, especially from around burned areas and the neck. Burned areas swell rapidly. Cover the area of the burn. Use a cool, moist bandage or a clean cloth. Don't immerse large severe burns in water. Doing so could cause a serious loss of body heat (hypothermia). Elevate the burned area. Raise the wound above heart level, if possible. Watch for signs of shock. Signs and symptoms include fainting, pale complexion or breathing in a notably shallow fashion. Treating minor burns For minor burns: Cool the burn. Hold the burned area under cool (not cold) running water or apply a cool, wet compress until the pain eases. Remove rings or other tight items from the burned area. Try to do this quickly and gently, before the area swells. Don't break blisters. Fluid-filled blisters protect against infection. If a blister breaks, clean the area with water (mild soap is optional). Apply an antibiotic ointment. But if a rash appears, stop using the ointment. Apply lotion. Once a burn is completely cooled, apply a lotion, such as one that contains aloe vera or a moisturizer. This helps prevent drying and provides relief. Bandage the burn. Cover the burn with a sterile gauze bandage (not fluffy cotton). Wrap it loosely to avoid putting pressure on burned skin. Bandaging keeps air off the area, reduces pain and protects blistered skin. If needed, take an over-the-counter pain reliever, such as ibuprofen (Advil, Motrin IB, others), naproxen sodium (Aleve) or acetaminophen (Tylenol, others).

A walk through of an interactive about male to female sex reassignment surgery.

Treatment consists of diet modifications and laxatives A high-fiber diet can be effective, along with over-the-counter medications, such as stool softeners. In some cases, a medical procedure to remove the hemorrhoid may be needed to provide relief.
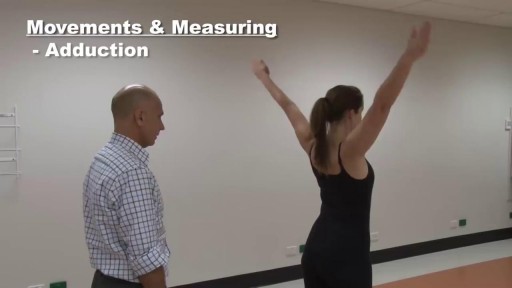
houlder examination frequently appears in OSCEs. You’ll be expected to pick up the relevant clinical signs using your examination skills. This shoulder examination OSCE guide provides a clear step by step approach to examining the shoulder, with an included video demonstration.

Fillings are a way for dentists to restore a partially decayed tooth. While many people fear the dentist, this procedure is typically quick, effective, and inexpensive. Without fillings, cavities can rapidly worsen. Seeing a dentist regularly can help you to monitor the condition of your teeth and plan for corrective procedures. According to the National Institute of Dental and Craniofacial Research, nearly 93 percent of adults between the ages of 20 and 64 have cavities, and at least 29 percent have decay that is untreated. Dentists can quickly identify tooth decay and then come up with a plan of action that involves filling teeth and restoring adverse conditions. You can do your part by sticking to a solid at-home oral hygiene routine. By simply brushing twice a day with a fluoride-treated toothpaste and flossing regularly, you can prevent the build up of bacteria-rich plaque and eliminate cavity-causing conditions.
