- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Of the many factors that affect your compatibility with a man, one of the biggest (or smallest) is in his pants. As with humour, interests or habits, the wrong fit can leave you cold. Or traumatised. In a study of 1,661 penises, Dr Debby Herbenick, author of Sex Made Easy, found an almost nine-inch difference in erection size: from 1.6 inches to 10.2. And since absolutely nothing outside the package tells you what to expect with the package, you have to test compatibility the hard way. Sometimes you hit your jackpot, sometimes it's just fine, and sometimes he's the guy on either end of that erection spectrum. These writers have been there, so here's what they learned - and how you can deal (without the gasp reflex).
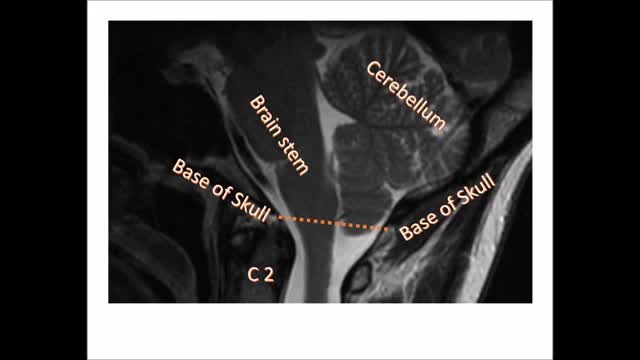
Chiari malformation (kee-AH-ree mal-for-MAY-shun) is a condition in which brain tissue extends into your spinal canal. It occurs when part of your skull is abnormally small or misshapen, pressing on your brain and forcing it downward.
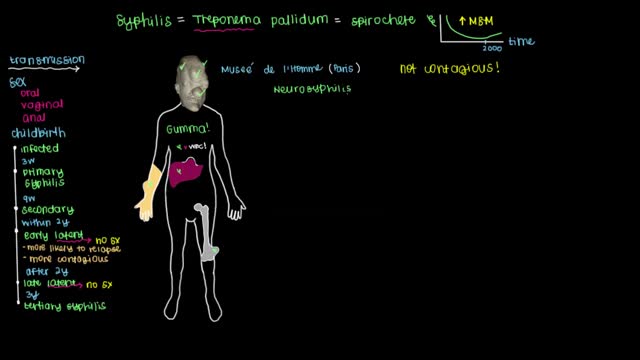
Syphilis develops in stages, and symptoms vary with each stage. But the stages may overlap, and symptoms don't always occur in the same order. You may be infected with syphilis and not notice any symptoms for years.

In the Womb - Identical Twins
Your kidneys are two bean-shaped organs that lie just below your rib cage, on each side of your spine. They remove waste from your body, level out your blood pressure, and keep your bones strong. They also ensure that you have the right amount of chemicals, like potassium and sodium (salt), in your blood. Finally, they make the hormone that causes your body to create red blood cells.

Aim: To detail two different clinical protocols and case studies using mini-implant anchorage developed to respond to certain clinical conditions. Methods: Two clinical protocols are described to upright mesially tilted mandibular molars. In the first protocol, a single mini-implant is inserted distally to the molar to be uprighted, and an elastic traction chain is applied to the tooth. In the second clinical approach, two mini-implants are inserted mesially. A screw-suspended TMA sectional archwire is applied (Derton-Perini technique). Two cases, descriptive of the two different treatment protocols, are described. In the first case, the mandibular right second premolar was missing and the adjacent first molar needed to be uprighted. A single screw was inserted distally to the first molar, and an elastic chain was applied. In the second case, the mandibular left second molar was missing and the third molar needed to be uprighted. Two mini-implants were inserted mesially and a fully screw-supported sectional archwire was used to upright and bodily mesialize the third molar. Results: Both uprighting approaches uprighted the molar axis without loss of anchorage. Conclusion: The two approaches to mandibular molar uprighting, developed as rational responses to different clinical cases, were both found to be effective. Research paper: Mandibular molar uprighting using mini-implants: Different approaches for different clinical cases-Two case reports.. Available from: https://www.researchgate.net/publication/224920305_Mandibular_molar_uprighting_using_mini-implants_Different_approaches_for_different_clinical_cases-Two_case_reports [accessed
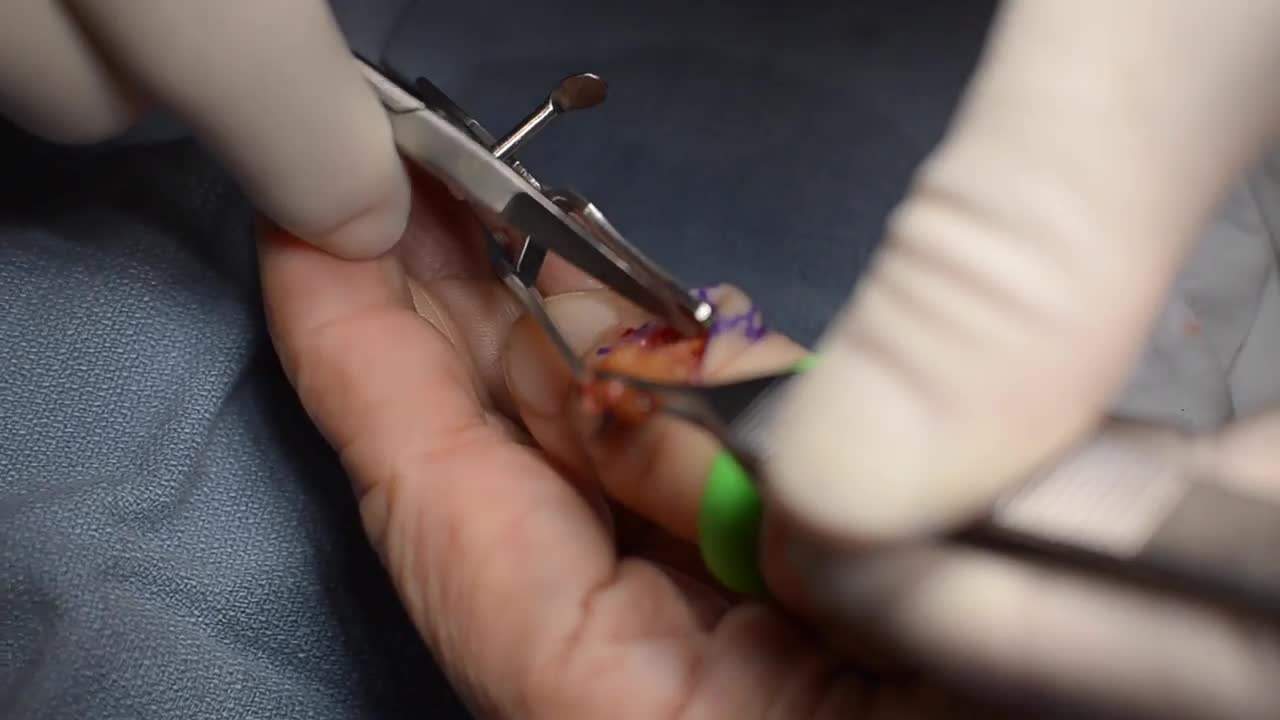
GIANT CELL TUMOR REMOVAL Plastic, Cosmetic and Reconstructive
Parasitic twins: boy carrying dead twin inside him, giant tumor removed - tumors compilation
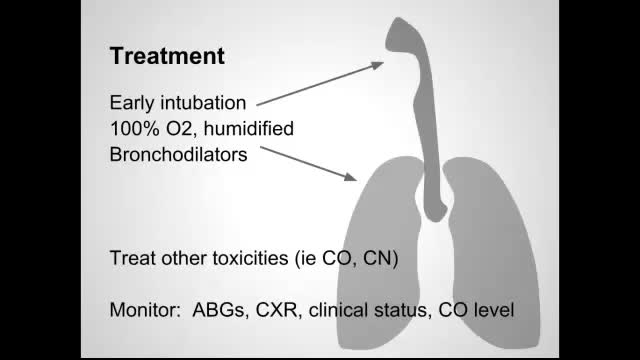
Smoke inhalation is the leading cause of death due to fires. It produces injury through several mechanisms, including thermal injury to the upper airway, irritation or chemical injury to the airways from soot, asphyxiation, and toxicity from carbon monoxide (CO) and other gases such as cyanide.

People whose back or neck pain has not been relieved by back surgery or other treatments may have another option to consider: spinal cord stimulation. Around the world, some 14,000 patients undergo spinal cord stimulator implants each year. Spinal cord stimulation (SCS) delivers mild electrical stimulation to nerves along the spinal column, modifying or blocking nerve activity in a non-medicinal way to minimize the sensation of pain reaching the brain.
Most people with TS are not significantly impaired by their symptoms and therefore do not require treatment with medication. However, several medications are available to control TS symptoms that interfere with functioning. Except in more severe cases when tics are sometimes painful, the main reasons for medication are to improve appearance and lessen embarrassing social interactions. As with all medications, there are possible side effects that should be monitored carefully by the physician. Patients should always be included in the decision to take medication, as they are the best judge of how disruptive the symptoms are to them. Early diagnosis and treatment are crucial to help the person with TS cope with his or her condition. Often, people make fun of a person with TS. Parents of children with TS also may find it difficult to cope with their child's behavior. When people with TS are diagnosed correctly and treated for the condition early, they can learn to cope with their disorder and accept that they are ok and normal.

The cause for TS is unknown. Early research suggested that TS is an inherited condition (often, the person's near or distant relatives have had some form of transient or chronic tic disorder or associated symptoms). Recent studies point to a combination of environmental and genetic factors as a cause of the disorder. The specific genes involved in the development of TS are still being investigated. Studies suggest that TS has a neurological basis and results from an abnormality which affects the brain's metabolism of certain neurotransmitters (chemicals in the brain that regulate behavior.) Current research being funded by the Tourette Syndrome Association (TSA) will help provide more information about the causes and genetic factors of TS.

Simple interrupted suturing is the most basic and most important of the suturing techniques.
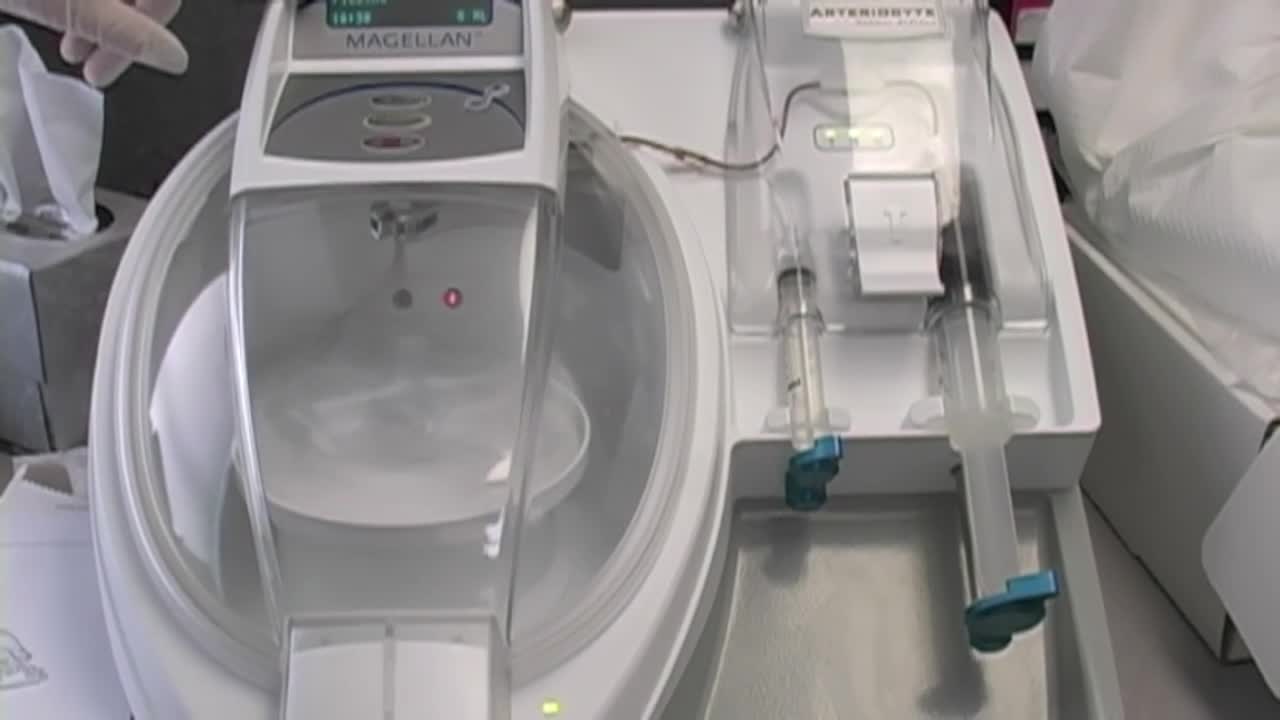
Stem Cell Injection Treatment - Stem Cell Therapy

Would you dare to explore your heritage? WIN a DNA kit and discover just how diverse you really are.
Alcoholic liver disease is a term that encompasses the liver manifestations of alcohol overconsumption, including fatty liver, alcoholic hepatitis, and chronic hepatitis with liver fibrosis or cirrhosis. It is the major cause of liver disease in Western countries.
Hypertrophic pyloric stenosis (HPS) causes a functional gastric outlet obstruction as a result of hypertrophy and hyperplasia of the muscular layers of the pylorus. In infants, HPS is the most common cause of gastric outlet obstruction and the most common surgical cause of vomiting.

Sialadenitis is an infection of the salivary glands. It is usually caused by a virus or bacteria . The parotid (in front of the ear) and submandibular (under the chin) glands are most commonly affected. Sialadenitis may be associated with pain, tenderness, redness, and gradual, localized swelling of the affected area.

Gallbladder cancer is cancer that begins in the gallbladder. Your gallbladder is a small, pear-shaped organ on the right side of your abdomen, just beneath your liver. The gallbladder stores bile, a digestive fluid produced by your liver. Gallbladder cancer is uncommon. When gallbladder cancer is discovered at its earliest stages, the chance for a cure is very good. But most gallbladder cancers are discovered at a late stage, when the prognosis is often very poor. Gallbladder cancer is difficult to diagnose because it often causes no specific signs or symptoms. Also, the relatively hidden nature of the gallbladder makes it easier for gallbladder cancer to grow without being detected. Symptoms ShareTweet Aug. 07, 2014 References Products and Services Book: Mayo Clinic on Digestive Health Give today to find cancer cures for tomorrow See also Abdominal pain Can you recommend a diet after gallbladder removal? Chemo Targets Chemotherapy Chemotherapy and hair loss: What to expect during treatment Chemotherapy and sex: Is sexual activity OK during treatment? Chemotherapy nausea and vomiting: Prevention is best defense Show more Advertisement Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission. Advertising & Sponsorship PolicyOpportunitiesAd Choices Mayo Clinic Store Check out these best-sellers and special offers on books and newsletters from Mayo Clinic. NEW! – The Mayo Clinic Diet, Second Edition Relief for America's epidemic of indigestion Keeping your bones healthy and strong Manage blood pressure for better health The Mayo Clinic Diet Online

3D Printed Models Used in the Mayo Clinic's First Face Transplant
