- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Tighten Sagging Breasts
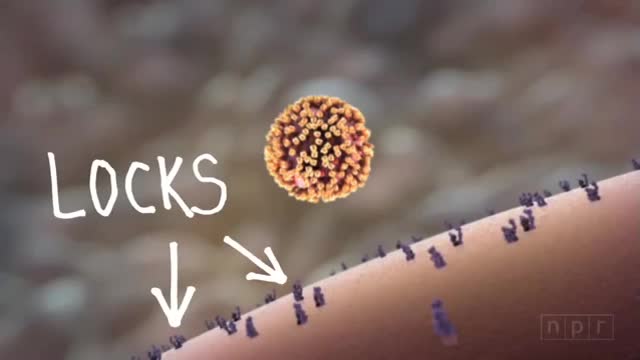
There are two main types of influenza (flu) virus: Types A and B. The influenza A and B viruses that routinely spread in people (human influenza viruses) are responsible for seasonal flu epidemics each year. Influenza A viruses can be broken down into sub-types depending on the genes that make up the surface proteins. Over the course of a flu season, different types (A & B) and subtypes (influenza A) of influenza circulate and cause illness.


Glomus tumors are rare soft tissue neoplasms that typically present in adults (ages 20-40 years) as small, blue-red papules or nodules of the distal extremities, with most cases involving subungual sites. These tumors are typically painful, often causing paroxysmal pain in response to temperature changes or pressure. Glomus tumors are thought to arise from the glomus body, a thermoregulatory shunt concentrated in the fingers and toes. Most lesions are solitary and localized to cutaneous sites; however, generalized glomuvenous malformations, or multiple glomangiomas, have also been described, and may have extracutaneous involvement.

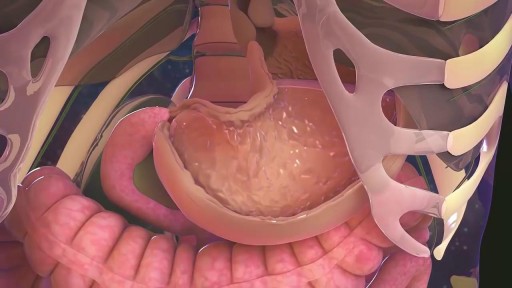
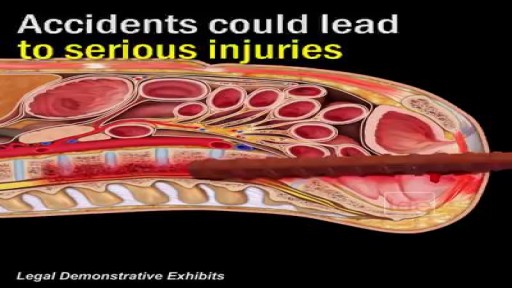
A hiatal hernia occurs when the upper part of the stomach pushes through an opening in the diaphragm and into the chest cavity. The diaphragm is the thin muscle wall that separates the chest cavity from the abdomen. The opening in the diaphragm is where the esophagus and stomach join.

Cerclage is indicated in a patient with a history of painless cervical dilation and a second trimester loss. It is also indicated in a patient with a history of preterm birth and a short cervix found on ultrasound between 16-24 weeks gestation. Cerclage placement occurs after the first trimester in case the pregnancy is genetically abnormal and would likely result in a first trimester loss.
Rectal bleeding can refer to any blood that passes from your anus, although rectal bleeding is usually assumed to refer to bleeding from your lower colon or rectum. Your rectum makes up the last few inches of your large intestine. Rectal bleeding may show up as blood in your stool, on the toilet paper or in the toilet bowl. Blood that results from rectal bleeding can range in color from bright red to dark maroon to a dark, tarry color.
A hemangioma (he-man-jee-O-muh) is a birthmark that most commonly appears as a rubbery, bright red nodule of extra blood vessels in the skin. A hemangioma grows during the first year of life, and then recedes over time. A child who had a hemangioma during infancy usually has little visible trace of the growth by age 10.
Many people report that inversion table therapy is a great way to stretch muscles and ligaments, reduce muscle spasms, and improve circulation. Stretching stimulates the lymph glands to increase the flow of lymphatic fluids; part of the body's waste disposal system. Similarly, cellular health depends on good blood circulation to deliver nourishment and remove waste. Inversion table therapy also helps to relieve motion sickness and stress. In addition, the body becomes more aware of its spatial orientation and balance when the inner ear is stimulated during inversion. Plus, it is not necessary for the body to be positioned completely upside down to gain benefits from inversion therapy! Unlike antigravity boots used with an inversion rack, an adjustable inversion table offers the flexibility to choose the most comfortable angle. Dialogue with Your Doctor Like anything that can affect your health, talk to your doctor before you start using an inversion table. This is important because certain medications and health conditions may make using an inversion table unsafe. Your doctor may recommend against inversion table therapy if you have obesity, a detached retina, fracture, glaucoma, heart condition (circulatory problem), hernia, implanted device, middle ear or eye infection, osteoporosis, are pregnant, or have a spinal injury. There may be other medical conditions not listed that your doctor may view as a contraindication.
http://angularcheilitis-end.cbwin1.com Corner Of Mouth Cracked, Angular Cheilitis, Home Remedies For Angular Cheilitis, Angular Cheilitis How to Treat Angular Cheilitis Effectively Thousands or even millions of people are searching every year for an effective treatment that will get them rid for good of Angular Cheilitis. Some manage to relieve themselves from the pains this skin conditions causes, while others continue to struggle for months with this terrible skin condition. For those who are still trying to get rid of Angular Cheilitis but still have not yet found a good result, here are some tips which may make your fight easier. As you probably know, the first thing you have to do when the first signs of Angular Cheilitis appear is to discover the cause which determined the apparition of this skin condition. You can make an examination of the area and see if there have been folds where moisture could be retained. If you have had some teeth pulled out or if you are wearing dentures, such folds may appear in time. If this is the issue, you should fix that by making an appointment to your dentist. Also, some blood tests will show you if your body has all the nutrients and vitamins it needs to function properly. In most of the cases, the Angular Cheilitis is triggered by malnutrition and anemia, thus making these tests will help you see whether this is your case, too. Once you know the results of the blood tests you should know if you should take vitamin supplements or your Angular Cheilitis was only a surface problem, caused by excessive moisture in the corners of your mouth. Apart from addressing the problem from the interior to the exterior, you will also have to apply some creams or ointments which will alleviate your suffering and at the same time will actively work on the sores. What most Angular Cheilitis treatments do is create a dry environment in which the bacteria cannot develop and trap them between the layer of cream and the layer of skin, thus killing them. Hydrocortisone, Mycolog II cream (which contains triamcinolone acetonide and nystatin) and Miconazole are the most popular medications prescribed by dermatologists in such conditions.

A bodybuilder gets his shoulder leaking because of synthol use on the stage while posing back double biceps

There is any chance that the snake is venomous The person has difficulty breathing There is loss of consciousness If you know the snake is not venomous, treat as a puncture wound. 1. Note the Snake's Appearance Be ready to describe the snake to emergency staff. 2. Protect the Person While waiting for medical help: Move the person beyond striking distance of the snake. Have the person lie down with wound below the heart. Keep the person calm and at rest, remaining as still as possible to keep venom from spreading. Cover the wound with loose, sterile bandage. Remove any jewelry from the area that was bitten. Remove shoes if the leg or foot was bitten. Do not: Cut a bite wound Attempt to suck out venom Apply tourniquet, ice, or water Give the person alcohol or caffeinated drinks or any other medications
Check out @barrettplasticsurgery on TikTok!
Like and subscribe for more! #shorts #medical #plasticsurgery
More information:
www.drdanielbarrett.com
How To Help Your Child Learn To Read, Help My Child Learn To Read, Best Way To Teach Reading---- http://children-learning-reading.good-info.co -- how to help your child learn to read - Help My Child Learn to Read The ability to read is vital for success. It helps your child succeed in school, helps them build self-confidence, and helps to motivate your child. Being able to read will help your child learn more about the world, understand directions on signs and posters, allow them to find reading as an entertainment, and help them gather information. Learning to read is very different from learning to speak, and it does not happen all at once. There is a steady progression in the development of reading ability over time. The best time for children to start learning to read is at a very young age - even before they enter pre-school. Once a child is able to speak, they can begin developing basic reading skills. Very young children have a natural curiosity to learn about everything, and they are naturally intrigued by the printed texts they see, and are eager to learn about the sounds made by those letters. You will likely notice that your young child likes to look at books and thoroughly enjoys being read to. They will even pretend to behave like a reader by holding books and pretend to read them. As parents, you're the most important first step in your children's journey into the wonderful world of reading. It is up to you to create the most supportive environment that turns your child on to reading - such as reading aloud to them often during the day and before bedtime, and placing age appropriate books for children around the house, so that the child will have access to plenty of books. Reading often to your child will help develop their interest in books and stories, and soon they will want to read stories on their own. >>Teach your child to read and enable your child to become a fast and fluent reader! Click here to help your child learn to read http://children-learning-reading.good-info.co
Always remember: safety first. (Warning: Graphic)
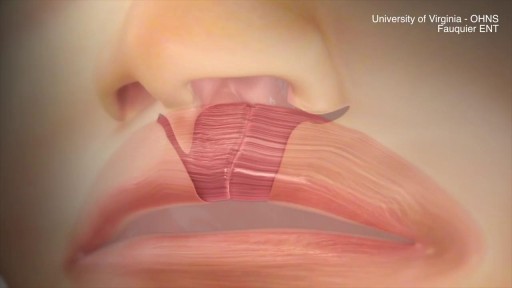
This animation demonstrates how a unilateral complete cleft lip repair is performed. This video is meant for educational purposes for patients and families. There are many ways to fix a complete cleft lip, but the technique shown here is the most common known as the Millard Rotation Advancement Repair.

Enchondroma (Cartilage) benign tumor of the finger.
