热门视频

Microcalcifications in the breast can be the first sign of cancer. They are, as the name says, very small and clustered. A precise biopsy without pain under stereotactic guidance is the standard procedure. What makes this Spirotome different from the vacuum assisted biopsies is that only a few biopsies are needed and that the approach of the needle towards the microcalcifications is direct and frontal. There is no damage to the surrounding tissues making this procedure rather painfree and with minimal bleeding.

Vasectomy is a minor surgical procedure wherein the vasa deferentia of a man are severed, and then tied or sealed in a manner such to prevent sperm from entering the seminal stream (ejaculate). Typically done in an outpatient setting, a traditional vasectomy involves numbing (local anesthetic) of the scrotum after which 1 (or 2) small incisions are made, allowing a surgeon to gain access to the vas deferens.

This video demonstrates Laparoscopic Cholecystectomy Fully Explained Skin-to-Skin Video with Near Infrared Cholangiography performed by Dr R K Mishra at World Laparoscopy Hospital. A laparoscopic cholecystectomy is a minimally invasive surgical procedure that involves removing the gallbladder. It is typically performed using small incisions in the abdomen, through which a laparoscope (a thin tube with a camera and light) and surgical instruments are inserted. The surgeon uses the laparoscope to visualize the inside of the abdomen and to guide the instruments in removing the gallbladder.
Near-infrared cholangiography is a technique that uses a special camera and fluorescent dye to visualize the bile ducts during surgery. The dye is injected into the cystic duct (the tube that connects the gallbladder to the bile ducts) and the camera detects the fluorescence emitted by the dye, allowing the surgeon to see the bile ducts more clearly.
The combination of laparoscopic cholecystectomy and near-infrared cholangiography has become a standard of care in many hospitals and surgical centers. It allows for a more precise and efficient surgery, reducing the risk of complications such as bile duct injury.
The use of indocyanine green (ICG) with near-infrared imaging during laparoscopic cholecystectomy has several advantages. Here are some of them:
Better visualization of the biliary anatomy: ICG with near-infrared imaging allows for better visualization of the biliary anatomy during surgery. This helps the surgeon identify important structures, such as the cystic duct and the common bile duct, and avoid injuring them.
Reduced risk of bile duct injury: With better visualization of the biliary anatomy, the risk of bile duct injury during surgery is reduced. Bile duct injury is a serious complication that can occur during laparoscopic cholecystectomy and can lead to long-term health problems.
Improved surgical precision: ICG with near-infrared imaging also improves surgical precision. The surgeon can better see the tissues and structures being operated on, which can help reduce the risk of bleeding and other complications.
Shorter operating time: The use of ICG with near-infrared imaging can shorten the operating time for laparoscopic cholecystectomy. This is because the surgeon can more quickly and accurately identify the biliary anatomy, which can help streamline the surgery.
Overall, the use of ICG with near-infrared imaging is a valuable tool in laparoscopic cholecystectomy that can improve surgical outcomes and reduce the risk of complications.
Like any surgical procedure, laparoscopic cholecystectomy (gallbladder removal) has potential complications. Here are some of the most common ones:
Bleeding: Bleeding during or after the surgery is a possible complication of laparoscopic cholecystectomy. Most cases are minor and can be easily controlled, but in rare cases, significant bleeding may require a blood transfusion or even additional surgery.
Infection: Any surgical procedure carries a risk of infection. After laparoscopic cholecystectomy, there is a risk of infection at the site of the incisions or within the abdomen. Symptoms may include fever, pain, redness, or drainage from the incision sites.
Bile leakage: In some cases, a small amount of bile may leak from the bile ducts into the abdominal cavity after gallbladder removal. This can cause abdominal pain, fever, and sometimes requires further surgery or treatment.
Injury to nearby organs: During the surgery, there is a small risk of unintentional injury to nearby organs such as the liver, intestines, or bile ducts. This can cause additional complications and may require further treatment.
Adverse reactions to anesthesia: As with any surgery requiring general anesthesia, there is a small risk of adverse reactions to the anesthesia, such as an allergic reaction, respiratory problems, or heart complications.
Most patients recover without complications following a laparoscopic cholecystectomy, but it is important to discuss any concerns or questions with your surgeon beforehand.
Contact us
World Laparoscopy Hospital
Cyber City, Gurugram, NCR Delhi
INDIA : +919811416838
World Laparoscopy Training Institute
Bld.No: 27, DHCC, Dubai
UAE : +971525857874
World Laparoscopy Training Institute
8320 Inv Dr, Tallahassee, Florida
USA : +1 321 250 7653
Regenerate response
Vaginal discharge serves an important housekeeping function in the female reproductive system. Fluid made by glands inside the vagina and cervix carries away dead cells and bacteria. This keeps the vagina clean and helps prevent infection. Most of the time, vaginal discharge is perfectly normal. The amount can vary, as can odor and hue (its color can range from clear to a milky white-ish), depending on the time in your menstrual cycle. For example, there will be more discharge if you are ovulating, breastfeeding, or are sexually aroused. The smell may be different if you are pregnant or you haven't been diligent about your personal hygiene. None of those changes is cause for alarm. However, if the color, smell, or consistency seems significantly unusual, especially if it accompanied by vaginal itching or burning, you could be noticing an infection or other condition. What causes abnormal discharge? Any change in the vagina's balance of normal bacteria can affect the smell, color, or discharge texture. These are a few of the things that can upset that balance:
Watch that video to know How to Avoid Pregnancy Without Using Condoms

An untreated hepatic abscess is nearly uniformly fatal as a result of complications that include sepsis, empyema, or peritonitis from rupture into the pleural or peritoneal spaces, and retroperitoneal extension. Treatment should include drainage, either percutaneous or surgical. Antibiotic therapy as a sole treatment modality is not routinely advocated, though it has been successful in a few reported cases. It may be the only alternative in patients too ill to undergo invasive procedures or in those with multiple abscesses not amenable to percutaneous or surgical drainage. In these instances, patients are likely to require many months of antimicrobial therapy with serial imaging and close monitoring for associated complications.

When diving into a Breast Reduction procedure, there are many things to consider. Even as a patient, being aware of any concerns and how the procedure works is important. Therefore, when a plastic surgeon operates on a patient, the results are clear. Dr. Linder, a Breast surgeon specialist in Beverly Hills, helps explain what goes into a Breast Reduction Procedure.
Understand how this world-class surgery platform operates a minimally invasive robotic surgery during a medical procedure for prostate cancer.

Join Dr. Parsia Vagefi, Chief of Surgical Transplantation and Dr. Steven Hanish, Surgical Director of Liver Transplantation, as they grant unprecedented access to the OR while performing a #Liver #Transplant #Surgery.
To find out more about UT Southwestern's transplant programs visit:
https://www.utswmed.org/transplant


Ever wonder what a drain is for after a Tummy Tuck? Here’s a short explanation by Dr. William.
#tummytuck #abdominoplasty #shorts

Resection of sigmoid colostomy prolapse

Dental Braces Animation

Neurosurgeon Sujit Prabhu, M.D., discusses what happens after surgery and how a patient recovers.
Learn more: http://www.mdanderson.org/educ....ation-and-research/d
Request an appointment at MD Anderson by calling 1-877-632-6789 or online: https://my.mdanderson.org/requestappointment

A 29 years old man lost his left wrist in car turn over in 2014. this video is taken 1 year after replantation. You can see another videos in my site: https://drliaghatclinic.com, https://instagram.com/liaghatclinic, https://t.me/liaghatclinic
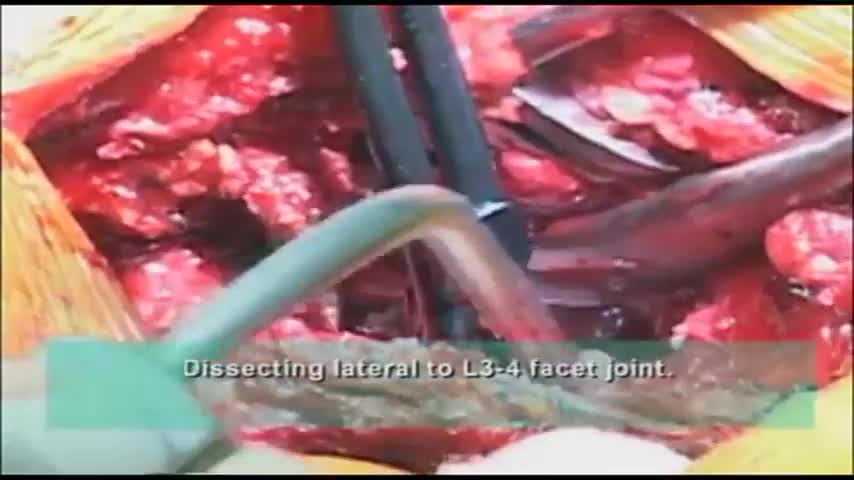
Surgeon performs a dissection of the transverse process during spine surgery, explaining the benefits of including the AQUAMANTYS System from Salient Surgical Technologies during the procedure. The AQUAMANTYS System uses Salient's patented TRANSCOLLATION technology, which has been clinically shown to reduce blood loss and lower blood transfusion rates when used during surgery.

For more than 25 years, The Children's Hospital of Philadelphia — the first Level 1 Pediatric Trauma Center in Pennsylvania — has provided unparalleled medical and surgical care for all injured children, including those with the most severe injuries.
Learn what makes the Trauma Center at CHOP a Level 1 Pediatric Trauma Center, and how our work toward trauma prevention, research advances and overall trauma awareness provides hope for reduced injuries in the future.
Learn more about the Trauma Center at CHOP: http://www.chop.edu/trauma.

@Samaritan Medical Center engaging in education and practicing skills are key. We are committed to programs that do just this. This October, all nursing staff attended the required Annual Skills Fair. Our amazing nursing team not only has a chance to learn and practice but also to network with their colleagues. Our Clinical Educators and Nurse Leaders organize the event and spend the time investing in your staff.
If you are interested in becoming part of the Samaritan nursing team, apply today: www.samaritanhealth.com/careers.
________________________________________

Eric's Home Dialysis

Tonsil Stones Caseum
