- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

This 35 years old man lost his right wrist in metal lathe cut machine. the video is taken about 2 years after replantation. You can see another videos in my site: https://drliaghatclinic.com, https://instagram.com/liaghatclinic, https://t.me/liaghatclinic

It depends upon which ligament is injured. If it is medial collateral ligament you feel pain when you walk ,sit and stand and you will be liming as well. If it is anterior cruciate ligament you feel pain when you walk on uneven ground.

Function and Anatomy: The hip is a ball and socket type joint, formed by the articulation of the head of the femur with the pelvis. Normal range of motion includes: abduction 45 degrees, adduction 20-30 degrees, flexion 135 degrees, extension 30 degrees, internal and external rotation. Hip pathology can cause symptoms anywhere around the joint, though frequently pain is anterior and radiates to the groin region. Additionally, pathology outside of the hip can be referred to this region. History and exam obviously help in making these distinctions.

Breast augmentation usually is performed in subglandular, subfascial, or partial submuscular pockets, including the dual plane. A new pocket has been described and used by the author. Methods: From October 2005 to April 2008, 600 patients underwent bilateral breast augme...
ntation using the new technique. Soft cohesive gel micro-textured round implants (range 200- 500cc) were used. The initial pocket is made in the subglandular plane up to the lower level of the nipple areolar complex. The submuscular plane is reached by splitting the pectoralis major muscle at the level of middle and lower third of sternum. The muscle is split along the direction of its fibers up and laterally to the anterior axillary fold. No pectoralis major is released from costal margin. The implant lies in this plane simultaneously behind and in front of the pectoralis major. Procedure is performed as a day case under general anesthetic with no drains. Results: Postoperative analgesia requirements is reduced because of dissection in natural planes resulting in quick recovery. No muscle contraction associated deformities is seen. All patients had aesthetically natural cleavage, with the nipple at the most projected part of the breast with three-dimensional enhancement. Conclusion: An adequate muscle cover of the prosthesis is achieved by muscle splitting breast augmentation technique and the procedure is used in all breast augmentations procedures

Cardiovascular Examination Clinical skills - Medical School Revision - Dr Gill
The cardiac exam is one of the clinical skills that medical students learn completely, as more often than not, patients will consult regularly about chest pain, and it is important to be able to identify key cardiovascular signs
As a junior doctor, the examination of the cardiovascular system can be almost a dreaded examination, as cardiac murmurs can literally take years of exposure in order to gain confidence with their identification through cardiac auscultation.
This video demonstrates not merely the examination of the heart, but the complete cardiovascular system including its peripheries.
I hope these clinical skill revision videos are helpful, please like and subscribe and join the community so that we can create more effective videos to help with your journey through medical school
#ClinicalExamination #ASMR #drgill
Some people have found this video useful for ASMR
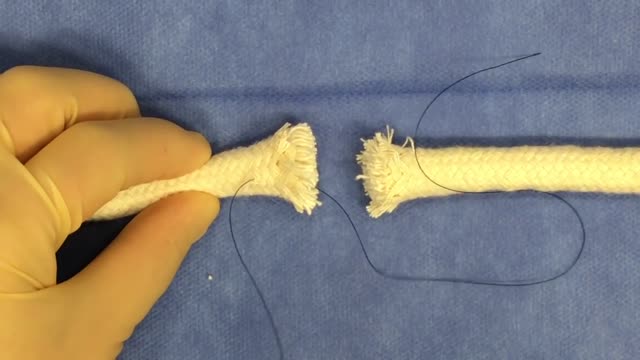
Tendon repair can be performed using: Local anesthesia (the immediate area of the surgery is pain-free) Regional anesthesia (the local and surrounding areas are pain-free) General anesthesia (the patient is asleep and pain-free) The surgeon makes a cut on the skin over the injured tendon. The damaged or torn ends of the tendon are sewn together. If the tendon has been severely injured, a tendon graft may be needed. In this case, a piece of tendon from the foot, toe, or another part of the body is often used. If needed, tendons are reattached to the surrounding tissue. The surgeon examines the area to see if there are any injuries to nerves and blood vessels. When the repair is complete, the wound is closed. If the tendon damage is too severe, the repair and reconstruction may have to be done at different times. The surgeon will perform one surgery to repair part of the injury, and then allow the hand to heal for a few weeks. Another surgery will be done later to complete the reconstruction and repair the tendon.
Endometrial Biopsy of Uterus
The uterus, or womb, is an important female reproductive organ. It is the place where a baby grows when a women is pregnant. There are different types of uterine cancer. The most common type starts in the endometrium, the lining of the uterus. This type of cancer is sometimes called endometrial cancer. The symptoms of uterine cancer include Unusual vaginal bleeding or discharge Trouble urinating Pelvic pain Pain during intercourse Uterine cancer usually occurs after menopause. Being obese and taking estrogen-alone hormone replacement therapy (also called menopausal hormone therapy) also increase your risk. Treatment varies depending on your overall health, how advanced the cancer is and whether hormones affect its growth. Treatment is usually a hysterectomy, which is surgery to remove the uterus. The ovaries and fallopian tubes are also removed. Other options include hormone therapy and radiation.

Shoulder Clinical Examination - Medical School Clinical Skills - Dr Gill
Personally, I find the shoulder examination the most complex examination possibly as there are so many variations and special tests. Some of which overlap and some will relate specifically to a patients presentation.
Often in a medical school syllabus, only select special tests will be used. In this shoulder exam demonstration, we include the Hawkins-Kennedy Test looking for impingement. This is dovetailed with examination for bicipital tendonitis as this is another possible cause of impingement type symptoms.
This shoulder upper limb exam follows the standard "Look, Feel, Move" orthopaedic exam approach, and overall order as set out in MacLeods Clinical Examination
Watch further orthopaedic examinations for your OSCE revision:
The Spine Examination:
https://youtu.be/pJxMHa6SCgU
Knee Examination
https://youtu.be/oyKH4EYfJDM
Hip Joint Clinical Examination
https://youtu.be/JC9GKq5nSdQ
________
Please note that there is no ABSOLUTE way to perform a clinical examination. Different institutions and even clinicians will have differing degrees of variations - the aim is the effectively identify medically relevant signs.
However during OSCE assessments. Different medical schools, nursing colleges, and other health professional courses will have their own preferred approach to a clinical assessment - you should concentrate on THEIR marks schemes for your assessments.
The examination demonstrated here is derived from Macleods Clinical Examination - a recognized standard textbook for clinical skills.
#ShoulderExamination #ClinicalSkills #DrGill

Palpation for Abdominal Masses

Testis operation
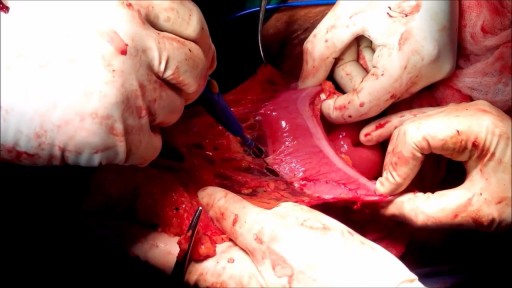
An omentectomy is a surgical procedure designed to remove the omentum, which is a thin fold of abdominal tissue that encases the stomach, large intestine and other abdominal organs. This fatty lining contains lymph nodes, lymph vessels, nerves and blood vessels.

External ring Invagination
Internal ring occlusion test
History Inspection Palpation
taxis
Zieman

Watch that video to know What is Vaginal Discharge and How To Get Rid of It

Tonsil Stones Caseum

Before Dr. Benjamin Carson became the first person to successfully separate twins conjoined at the head, before he had a TV movie made about his life, before he became known for his "gifted hands" and before he became head of pediatric neurosurgery at Johns Hopkins, Ben Carson was headed down the wrong path in life.
Watch that video to know What is Vaginal Discharge and How To Get Rid Of It?
top 10 most incredible surgeries ever done
Loyola oral Presentation for Rounds video
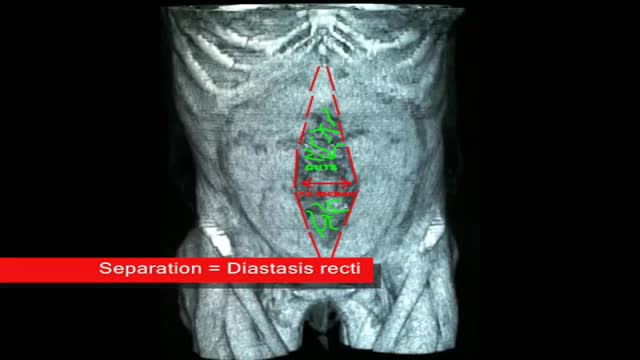
plastic surgeon demonstrates the results of a muscle separation(rectus diastasis) repair using 3 dimesional CAT scan and photographic images
