- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Most innovative dental implant system

Tuberous breast deformity is a congenital breast anomaly that becomes manifest at the time of puberty and breast development. The three components of tubular deformity usually include, pseudoherniation of breast tissue into the nipple areolar complex, poorly defined inframammary fold and flattening of the lower pole of the breast which leads to a conical tubular shape. Stuart Linder M.D. 9675 BRIGHTON WAY, SUITE 420 BEVERLY HILLS CA 90210 (310) 275-4513
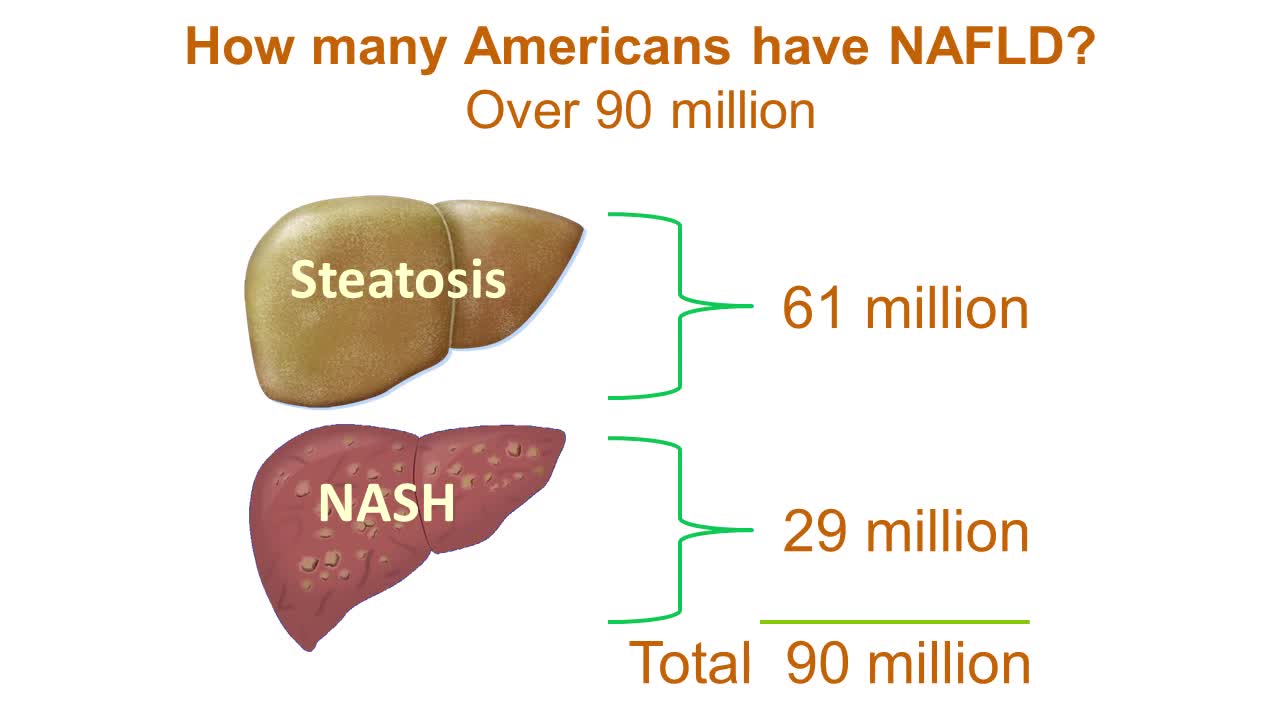
Nonalcoholic fatty liver disease is an umbrella term for a range of liver conditions affecting people who drink little to no alcohol. As the name implies, the main characteristic of nonalcoholic fatty liver disease is too much fat stored in liver cells. Nonalcoholic steatohepatitis, a potentially serious form of the disease, is marked by liver inflammation, which may progress to scarring and irreversible damage. This damage is similar to the damage caused by heavy alcohol use. At its most severe, nonalcoholic steatohepatitis can progress to cirrhosis and liver failure Nonalcoholic fatty liver disease is increasingly common around the world, especially in Western nations. In the United States, it is the most common form of chronic liver disease, affecting an estimated 80 to 100 million people. Nonalcoholic fatty liver disease occurs in every age group but especially in people in their 40s and 50s who are at high risk of heart disease because of such risk factors as obesity and type 2 diabetes. The condition is also closely linked to metabolic syndrome, which is a cluster of abnormalities including increased abdominal fat, poor ability to use the hormone insulin, high blood pressure and high blood levels of triglycerides, a type of fat. Nonalcoholic fatty liver disease care at Mayo Clinic Request an Appointment at Mayo Clinic Symptoms & causes Aug. 23, 2016 Print Share on: Facebook Twitter References Related Magnetic resonance elastography Nonalcoholic fatty liver disease Overview Symptoms & causes Diagnosis & treatment Diagnosis Treatment Departments & specialties Expertise & rankings Locations, travel & lodging Clinical trials Research Costs & insurance Preparing for your appointment Self-management More about In-Depth Multimedia Resources News from Mayo Clinic Advertisement

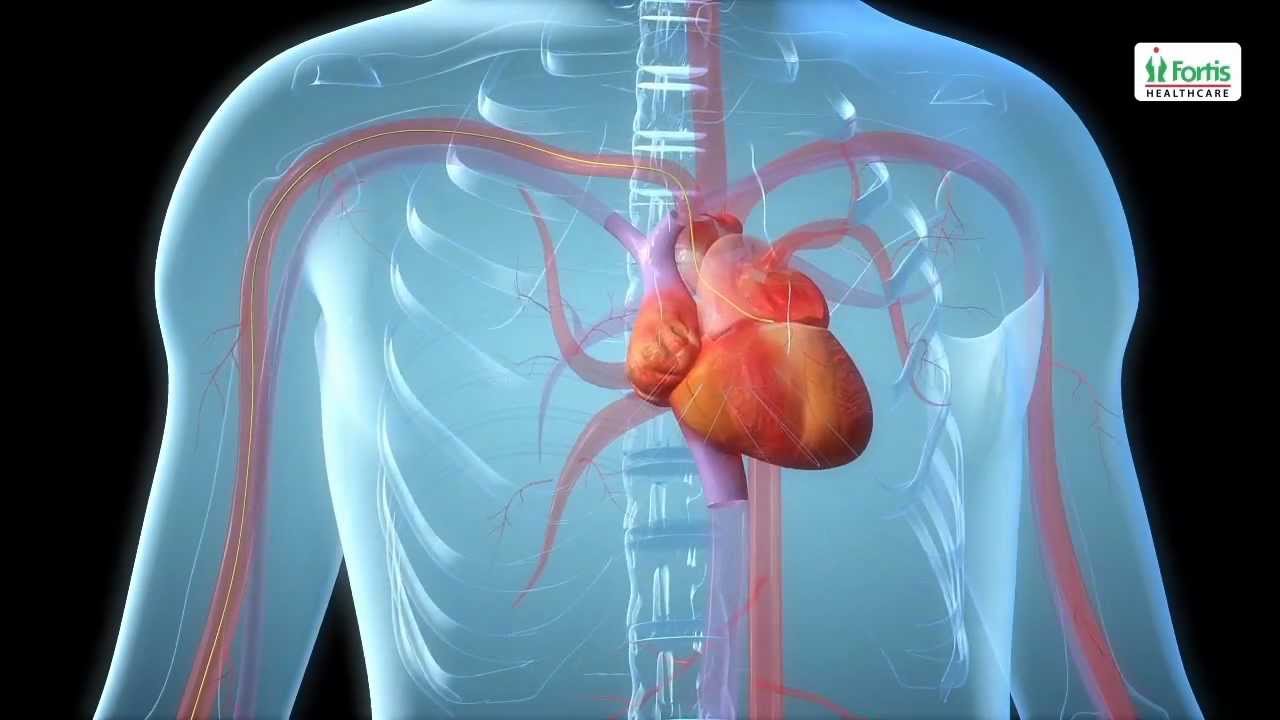
Angioplasty Procedure Animation Video
Emergency angioplasty is an operation that is performed directly after a heart attack, on admission to the hospital. It involves the insertion of a catheter into the blocked blood vessel that caused the heart attack. This opens it up and allows blood to flow again, thus minimizing damage to the heart.
If one or more arteries become clogged, it may result in a heart attack. This normally presents with chest pain, sweating and a feeling of anxiety, among other symptoms. Urgent medical assistance should be sought. A heart attack is a medical emergency requiring intervention as soon as possible.
Know more: http://www.emergencyangioplasty.com/
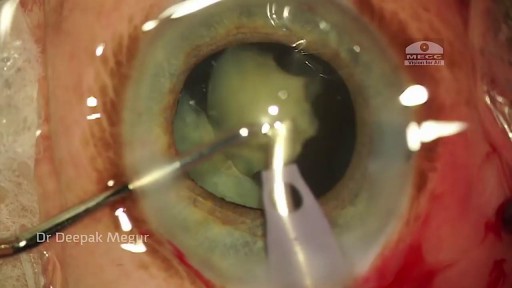
Phacolytic glaucoma usually is associated with a mature or hypermature cataract and typically occurs in elderly patients. Today, phacolytic glaucoma is rare in the United States, found primarily in areas where access to care is poor. Will the increase in the number of under- and uninsured patients lead to an increase in this condition? Evaluation and Diagnosis Signs and symptoms. Patients typically report acute-onset pain, decreased vision, tearing and photophobia. Examination will reveal injection, corneal edema, elevated IOP, anterior chamber reaction with or without pseudohypopyon, particles on the lens capsule and anterior capsule wrinkling. Patient history. The duration of symptoms should be elicited; a delayed presentation of more than five days since onset can result in glaucomatous disc damage and poorer prognosis.¹ The ocular history may reveal that the patient decided against removal of an advanced cataract. Prior intraocular surgery or trauma may have left residual lens material that could cause phacoanaphylactic glaucoma or exacerbate infectious endophthalmitis. Visual acuity and visual potential should be assessed. Exam essentials. A complete ophthalmologic examination should be done. The eye should be inflamed, and the cornea may be edematous due to the high IOP. The anterior chamber will demonstrate massive inflammation and/ or pseudohypopyon. Gonioscopy is essential; it will help rule out angle closure due to phacomorphic glaucoma or neovascularization of the angle. Assess ment of the posterior pole should be performed to rule out vitreous hemorrhage (which can result in ghost-cell glaucoma) or vitritis (which may be associated with infectious endophthalmitis or panuveitis). If the view to the fundus is obstructed, B-scan ultrasonography also should be performed. Differential diagnosis. The differential diagnosis includes infectious endophthalmitis, phacoanaphylactic glaucoma, inflammatory glaucoma, glaucoma secondary to intraocular tumor, phacomorphic glaucoma, acute-angle closure glaucoma and neovascular glaucoma. Management Medication. Medical management is used to temporarily control the glaucoma and inflammation. Initial treatment consists of hyperosmotic agents, aqueous suppressants, anti-inflammatory drugs and cycloplegics. Surgery. Definitive treatment is removal of the lens via extracapsular cataract extraction with or without an IOL. Some ophthalmologists defer placement of an IOL until after the inflammation subsides; however, there is no significant difference in final visual acuity between those patients who did receive an IOL and those who did not.¹ If the phacolytic glaucoma is of long duration (more than seven days), a combined trabeculectomy may be needed to prevent postoperative IOP spikes.² In eyes with hypermature Morgagnian cataracts, one must be especially careful, as the capsule is fragile, the zonules are weak and the view is difficult due to the white, milky cortex. Vision limited to light perception on presentation is not a contraindication to performing cataract extraction. Surgical Tips For a planned extracapsular cataract extraction with a posterior chamber IOL, fashion a superior fornix-based conjunctival flap.³ Make a partial-thickness incision along the sclerolimbal junction superiorly for 120 degrees with a No. 69 blade. Forty-five degrees away, a paracentesis should be done to decompress the eye. The anterior chamber fluid can be withdrawn for analysis, to look for macrophages and high molecular-weight proteins. Inject balanced salt solution in a cannula to wash out any residual particulate matter, then inject Healon or viscoelastic into the anterior chamber. Make an incision entering the anterior chamber at the 12 o’clock position with a keratome. A 26-gauge cystotome mounted on a syringe is then introduced through the 12 o’clock incision and used to puncture the capsular bag. The milky cortex should be aspirated as much as possible, until the nucleus is visible. Withdraw the needle through the keratome incision, then inject Healon through the 12 o’clock incision into the capsular bag. Next, enlarge the corneoscleral keratome incision with curved Westcott scissors to 120 degrees. Perform a partial V-shaped capsulotomy; this can be done either with the cystotome or with an angled Vannas scissors. Place viscoelastic under the nucleus to float the nucleus and sever any adhesions between the nucleus and the capsule. The nuclear portion of the lens can then be removed with an irrigating vectis (lens loop) with or without gentle pressure at the inferior limbus (6 o’clock). Irrigate and aspirate the residual cortex with the Simcoe cannula. Inspect the capsular bag; if it is intact, place a posterior chamber IOL into the bag. Close the incision with several interrupted 10-0 monofilament nylon sutures and reattach the conjunctival flap. Potential Sequelae and Prognosis Postoperatively, the patient should be managed with topical steroids and/or aqueous suppressants and hyperosmotics if necessary. Vitreous opacification behind the posterior capsule occurs in a small percentage of eyes. These vitreous opacities are typically absorbed by one to two weeks postoperatively. IOP usually is controlled without antiglaucoma medications after the cataract removal. A detailed glaucoma evaluation (including repeat gonioscopy to assess for peripheral anterior synechiae, visual field and optic nerve status) should be done to assess the extent of glaucomatous damage. The prognosis is dependent on the duration of elevated IOP, PAS and optic nerve damage. In one study, patients who were older than 60 and whose glaucoma was present for more than five days did significantly worse than a comparison group of younger individuals with shorter disease duration.


Complete examination of the back

In as many as 80% of cases, doctors don’t find the exact reason for a curved spine. Scoliosis without a known cause is what doctors call “idiopathic.” Some kinds of scoliosis do have clear causes. Doctors divide those curves into two types -- structural and nonstructural. In nonstructural scoliosis, the spine works normally, but looks curved. Why does this happen? There are a number of reasons, such as one leg’s being longer than the other, muscle spasms, and inflammations like appendicitis. When these problems are treated, this type of scoliosis often goes away.

Foley Catheter Insertion
A central venous catheter, also called a central line, is a long, thin, flexible tube used to give medicines, fluids, nutrients, or blood products over a long period of time, usually several weeks or more. A catheter is often inserted in the arm or chest through the skin into a large vein.
http://eliminar-seu-diabetes.good-info.co/ Tipos De Diabetes, Diabets, Alimentação Para Diabéticos, Diabetes Tipo Ii, Yacon Diabetes, https://youtu.be/iDK8jKuR_VQ É provável que se sinta identificado com alguma destas situações. Tem medo de uma complicação a longo prazo, como a perda da visão, a amputação dos dedos dos pés, de extremidades ou inclusive da morte? Quer terminar com as injeções diárias de insulina e as picadas nos dedos? Enfrenta diariamente o fato de que tem 80% de probabilidades de morrer com doenças cardíacas ou derrame cerebral? Sofre de excesso de peso que não pode eliminar, causada por seus medicamentos? Quer deixar de se sentir culpado por ter dietas especiais que complicam a organização da sua família? Está oprimido pelo cuidado e controle que diariamente esta doença precisa? Quer deixar de sofrer os terríveis efeitos secundários que provocam os medicamentos para o Diabetes? Sei o que se sente. pensar que não existe esperança, que não tem cura e que estamos condenados a viver doentes. Mas hoje Tenho Excelentes Notícias para lhe dar e posso garantir que o que você vai ler neste site será o mais importante que tenha lido em toda a sua vida.
Que Es Bueno Para La Diabetes Medicina Natural. Porque Con Este Método Que Voy a Revelarte que es 10 Veces Más Efectivo Que Cualquier Otro Podrás Vencer A Tu Diabetes RÁPIDAMENTE. Si no hubiera sido por el poderoso método inusual pero PROBADO que usé para obtener RESULTADOS rápidos y controlar la diabetes. La genialidad de este gran descubrimiento es que está diseñado para controlar, frenar y vencer a la diabetes. con la “complicidad” de tu propio cuerpo que se auto regenera si se le instalan los comando correctos en el metabolismo. Sin importar si tienes 7 ó 90 años. Sin importar si tu nivel de azúcar es más incontrolable que un caballo salvaje, o tu tipo de diabetes. Sin importar cuantas veces tu doctor te ha dicho que la diabetes no tiene cura. Sin importar si has fallado una docena de veces con tratamientos, medicamentos o métodos convencionales que NO SIRVEN. Estás a punto de descubrir cómo controlar la diabetes usando la Solución Natural más exitosa jamás revelada que transformará tu cuerpo en una máquina generadora de salud y energía – ¡en tan solo unos pocos días! haciendo click aqui. http://vencer-la-diabetes-rapido.info-pro.co

demonstrates how the Epley maneuver is performed to treat POSTERIOR canal BPPV affecting the right ear. Animation showing what is going on within the inner ear is also shown in the 2nd half of the video.
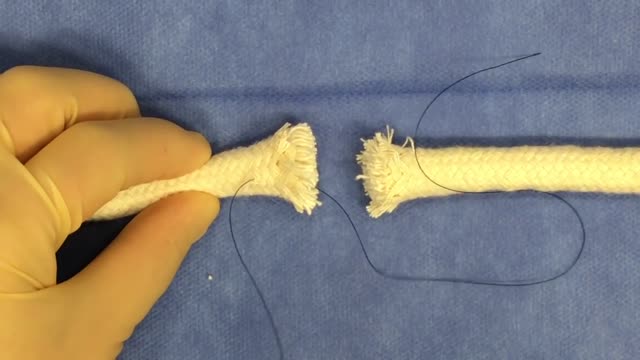
Tendon repair can be performed using: Local anesthesia (the immediate area of the surgery is pain-free) Regional anesthesia (the local and surrounding areas are pain-free) General anesthesia (the patient is asleep and pain-free) The surgeon makes a cut on the skin over the injured tendon. The damaged or torn ends of the tendon are sewn together. If the tendon has been severely injured, a tendon graft may be needed. In this case, a piece of tendon from the foot, toe, or another part of the body is often used. If needed, tendons are reattached to the surrounding tissue. The surgeon examines the area to see if there are any injuries to nerves and blood vessels. When the repair is complete, the wound is closed. If the tendon damage is too severe, the repair and reconstruction may have to be done at different times. The surgeon will perform one surgery to repair part of the injury, and then allow the hand to heal for a few weeks. Another surgery will be done later to complete the reconstruction and repair the tendon.

A bodybuilder gets his shoulder leaking because of synthol use on the stage while posing back double biceps

SUBSCRIBE: https://www.youtube.com/c/TVNe....phrologist?sub_confi
An animation of blood flow inside the Hemodialysis circuit.
About Dr. Rifai:
Dr. Ahmad Oussama Rifai is certified by the American Board of Internal Medicine (ABIM) in the specialty of Internal Medicine and the sub-specialty of Nephrology.
MEET DR. RIFAI
https://www.thevirtualnephrologist.com/rifai/
Follow The Virtual Nephrologist on SOCIAL MEDIA:
-Facebook: https://www.facebook.com/thevirtualnephrologist
-Instagram: https://www.instagram.com/thevirtualnephrologist/
-Twitter: https://twitter.com/VNephrologist
Schedule a virtual consult:
https://www.thevirtualnephrolo....gist.com/schedule-a-
Best wishes for great health | The Virtual Nephrologist
Loyola oral Presentation for Rounds video

Breast augmentation usually is performed in subglandular, subfascial, or partial submuscular pockets, including the dual plane. A new pocket has been described and used by the author. Methods: From October 2005 to April 2008, 600 patients underwent bilateral breast augme...
ntation using the new technique. Soft cohesive gel micro-textured round implants (range 200- 500cc) were used. The initial pocket is made in the subglandular plane up to the lower level of the nipple areolar complex. The submuscular plane is reached by splitting the pectoralis major muscle at the level of middle and lower third of sternum. The muscle is split along the direction of its fibers up and laterally to the anterior axillary fold. No pectoralis major is released from costal margin. The implant lies in this plane simultaneously behind and in front of the pectoralis major. Procedure is performed as a day case under general anesthetic with no drains. Results: Postoperative analgesia requirements is reduced because of dissection in natural planes resulting in quick recovery. No muscle contraction associated deformities is seen. All patients had aesthetically natural cleavage, with the nipple at the most projected part of the breast with three-dimensional enhancement. Conclusion: An adequate muscle cover of the prosthesis is achieved by muscle splitting breast augmentation technique and the procedure is used in all breast augmentations procedures
What is hemodialysis and how does it work? Who needs it? How do you prepare for it? In the United States, over 30 million Americans have kidney disease, and sometimes, kidney disease progresses to kidney failure or end-stage renal disease. When this happens, you cannot survive unless you have a kidney transplant or some form of dialysis. So today we're going to talk about hemodialysis.
Your kidneys are the two kidney bean-shaped organs that are located in your lower back, or in your flanks. And the kidneys are responsible for filtering out or cleaning your blood. They get rid of excess waste, excess toxins, and excess fluids. If your kidneys stop functioning, then you develop renal failure or end-stage renal disease.
What is Hemodialysis?
Hemodialysis, or blood dialysis, is the filtering of your blood outside of your body. So, if your kidneys stop working properly, the hemodialysis acts as a substitute kidney. Now it's important to note that hemodialysis does not actually correct your own kidney function. It does not fix or treat your kidneys.
#hemodialysis #drfrita
What is The Dialyzer?
The dialyzer is actually the filter. It's the main powerhouse of the hemodialysis system, and it is what actually acts as the substitute kidney. In the dialyzer, you have these hollow fibers that run through it, and these fibers are bathed in something called dialysates, or dialysis fluid.
How Often Are Patients Treated With Hemodialysis?
Most patients who are on hemodialysis are on it between three and six hours, about three days a week, especially if they go to a center.
How Does Hemodialysis Work?
So when you are on dialysis, how does your blood get from your body to the hemodialysis machine and then back to your body? Well, it does so through tubes, and those tubes are connected to your access, and we'll talk about access in just a moment. But as far as the tubing, the tubing is connected to your body.
Types Of Hemodialysis Access
Arteriovenous Fistula or AV Fistula
The AV fistula is the gold standard as far as hemodialysis access is concerned because it gives you the most efficient hemodialysis and it is the least likely to be infected.
Arteriovenous Graft or AV Graft
The AV graft is very similar to the AV fistula in that you still have a surgically connected artery and a vein, usually in the arm, but in the case where if you have veins that are rather thin or arteries that are thin and maybe too weak in order to really give you a properly functioning, substantial AV fistula, then the vascular surgeon may opt to add an artificial material in order to make that shunt a little stronger, or little more durable. And so, an AV graft is another option for dialysis access.
Catheter
If you're in a situation where you need temporary dialysis, or if you have acute kidney injury, then you may have a temporary Vascath placed, and it's usually placed in a vein of the neck, the internal jugular vein, or it can be placed in the groin, or in the femoral vein.
Who Needs Hemodialysis Treatment?
How do you know if you need hemodialysis, and when is it time to prepare? Well, if you follow up with your kidney doctor (nephrologist) regularly, he or she will be watching your labs. They'll be able to see those signs of your kidneys not functioning properly.
