- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

This minimally invasive technique allows surgeons to remove skull base tumors as large as softballs through the nose, with less trauma to the brain and critical nerves than with a traditional craniotomy.
To learn more, please visit https://www.upmc.com/

For more information about Mohs surgery, please visit https://cle.clinic/3x7CRTy
Mohs surgery is a highly effective skin cancer removal procedure that takes just a few hours. It is most often used to treat basal cell and squamous cell carcinomas, the two most common skin cancers.
Chapters:
0:00 How effective is Mohs Surgery?
0:23 When is Mohs Surgery used?
0:50 How does Mohs Surgery work?
1:55 Does Mohs Surgery cure skin cancer?
2:06 How long is the recovery period after Mohs Surgery?
Resources:
Skins Cancer: https://cle.clinic/3G2MMM8
How Skin Cancer Is Found and Removed — At the Same Appointment: https://cle.clinic/3r9Wzu6
The Best Strategies To Reduce Your Risk of Skin Cancer: https://cle.clinic/38Bazqn
The information in this video was accurate as of 4.8.2022 and is for information purposes only. Consult your local medical authority or your healthcare practitioner for advice.
▶Share this video with others: https://youtu.be/aCV1UZ0Yj-o
▶Subscribe to learn more about Cleveland Clinic:
https://www.youtube.com/user/C....levelandClinic?sub_c
#ClevelandClinic #MohsSurgery #SkinCancer
From across the room, using controls and pedals—pediatric surgeons at Golisano Children’s Hospital are now able to operate on patients without even touching them. “It allows performances of deep surgeries in the pelvis or abdomen through tiny, little incisions as opposed to a traditional, large incision to get access to the areas where urologists often operate,” explained Dr. Rahman Abd-El-Barr, a pediatric urologist with Golisano Children’s Hospital of Southwest Florida.
The DaVinci robot is a robotic platform that allows surgeons to do minimally invasive surgery, leaving patients with smaller incisions and a quicker recovery. “This is important because it allows us to minimize recovery time, pain, bleeding with surgery, and especially with kids, it helps them to get back on their feet right away,” he said.
So when high school athlete, Reagan Rebeor found out she needed to have kidney surgery, she decided to have it robotically. “Thankfully, I did that because if not, I would have had a long scar down my stomach instead of small holes, small incisions. I had pain for three days, three or four days. Then after that, I was fine,” she said.
While it’s not an option for all pediatric surgeries, doctors say it can be very beneficial for teenage and adult patients needing reconstructive surgery. An option that allows patients a quicker and easier recovery.
View More Health Matters video segments at LeeHealth.org/Healthmatters/
Lee Health in Fort Myers, FL is the largest network of health care facilities in Southwest Florida and is highly respected for its expertise, innovation and quality of care. For more than 100 years, we’ve been providing our community with personalized preventative health services and primary care to highly specialized care services and robotic assisted surgeries. Lee Health - Caring People. Inspiring Care.
Visit LeeHealth.org
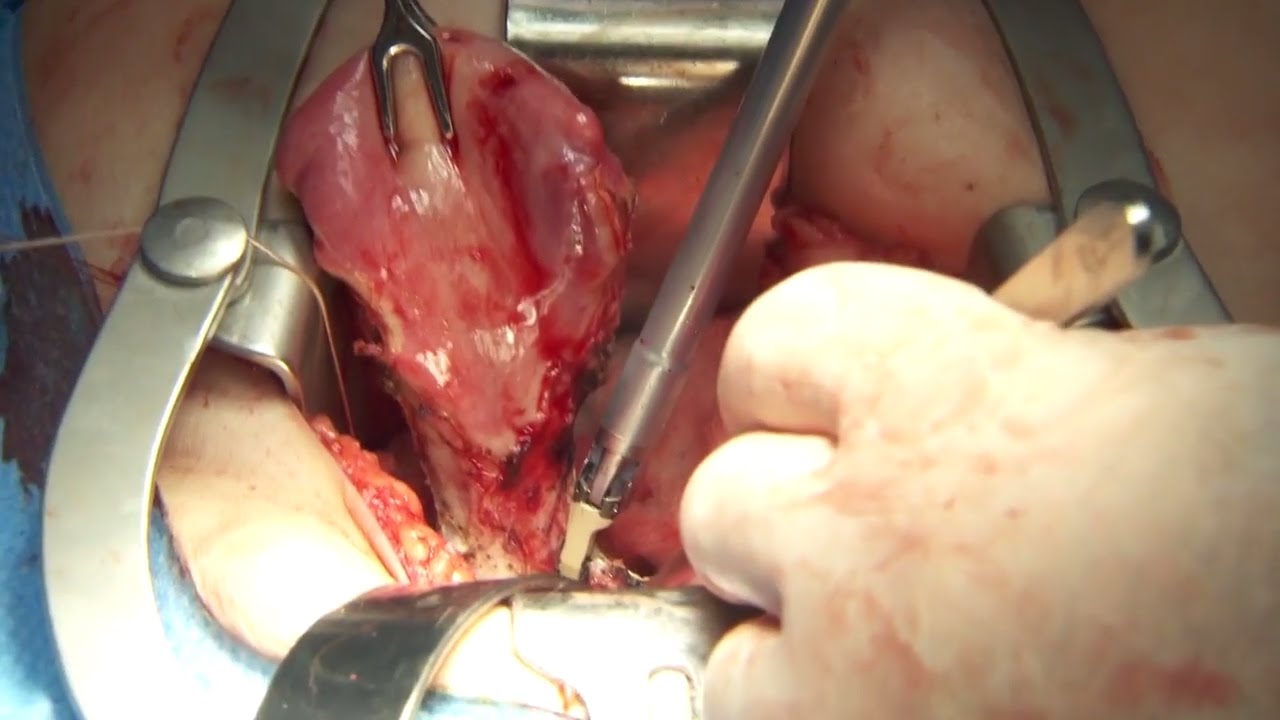
Olympus has extended the value of its award-winning combined surgical energy device, THUNDERBEAT, to open surgical procedures. Watch Dr. Francois Blaudeau master use of THUNDERBEAT Open Extended Jaw (OEJ) in a total abdominal hysterectomy.
http://medical.olympusamerica.com/products/thunderbeat?utm_source=youtube&utm_campaign=Total%20Abdominal%20Hysterectomy%20Surgery%20-%20THUNDERBEAT&utm_medium=description&utm_term=energy&utm_content=surgical

Be sure to have your teenager checked for hernias as they may be malevolent, Dr. Honaker gives us some insight as to why this is an important thing to have done.

@Samaritan Medical Center engaging in education and practicing skills are key. We are committed to programs that do just this. This October, all nursing staff attended the required Annual Skills Fair. Our amazing nursing team not only has a chance to learn and practice but also to network with their colleagues. Our Clinical Educators and Nurse Leaders organize the event and spend the time investing in your staff.
If you are interested in becoming part of the Samaritan nursing team, apply today: www.samaritanhealth.com/careers.
________________________________________

For Employees of Hospitals, Schools, Universities and Libraries: Download 8 FREE medical animations from Nucleus by signing up for a free trial: http://nmal.nucleusmedicalmedi....a.com/free-trial-mem
Biology students: Subscribe to the Nucleus Biology channel to see new animations on biology and other science topics, plus short quizzes to ace your next exam: https://bit.ly/3lH1CzV
This medical animation depicts Laser Eye Surgery, a procedure that permanently changes the shape of the cornea, the clear covering over the front of the eye.
#lasik #eye #cornea
ANCE00185

At Hologic, we are committed to delivering innovative educational tools and programming that empower you to deliver life-changing care. Learn more about us at Hologic.com.

Eric's Home Dialysis

#anatomy #histology #bytesizemed
✨If you would like my help studying about cartilage, you can check out my long-form video linked at the bottom of the screen.
💫 For more videos like this, subscribe to my channel, Byte Size Med.
📚Factual References & for Further Reading:
- DiFiore's Atlas of Histology
- Junqueira's Basic Histology
- Gartner's Concise Histology
- Openstax Anatomy and Physiology
https://openstax.org/details/b....ooks/anatomy-and-phy
- Openstax Biology
https://openstax.org/details/books/biology-2e
(The last two are links to open-source references. They are NOT affiliate links)
🌤 Note:
These are just a collection of my notes. So use them the way you would use borrowed notes from a friend. 📝
The images in this video are hand-drawn for illustration and explanation only.✍️ Hence, they may not be anatomically accurate. I am just one person making these videos. If there are any errors, that is unintentional. I try super hard to avoid them. Please let me know if you find any, so it gets clarified for other viewers. Science constantly evolves and changes. New discoveries are made everyday. So some of the information in these videos may become outdated. If you notice that, please let me know so I can update them.
⚡️Disclaimer:
These videos are NOT a substitute for a medical textbook. Textbooks are written by experts (which I do not claim to be), edited, proofread and referenced. Please use them.
The information has been sourced from multiple references as mentioned above. I draw all the pictures myself. But if I have inadvertently infringed on any copyright, that is completely unintentional. I only make these videos to impart education. If I have accidentally violated copyright in any way, do let me know so I can make the necessary changes or give credit to anyone who is owed the same.
These videos are NOT intended for patient education. They are NOT a substitute for diagnosis and treatment by a licensed medical professional. Always seek the advice of a qualified health care provider for any questions you may have regarding any medical condition, so that they can address your individual needs.
🔅They are ONLY meant to help students of medicine and health sciences with studying, and should be used for just that purpose and absolutely nothing else.
Byte Size Med. All Rights Reserved.

**PLEASE READ FULLY
Purpose of the video is to help Esthetician’s review chapters in their text book to better prepare for State Bord testing, by simply reading and going over some of the material, it’s not intended to replace any teaching from any Beauty College. Every instructor does things different, Keep in mind I am in the state of Texas, also keep in mind that when in school students are to follow guidelines and might be required to do things a bit different, I teach my students the text book because that is where the state board questions come from and the goal is for them to pass their board exams. I also teach them and go over real working situations they might come across in the salon or spa.
* I am not affiliated with TDLR or PSI in any way
PSI Bulletin Link
https://candidate.psiexams.com/bulletin/display_bulletin.jsp?ro=yes&actionname=83&bulletinid=173&bulletinurl=.pdf
Glymed store: https://glymedplus.io/home/index?store=0011298
email: glamandbeyondinfo@gmail.com

Ophthalmoscopy - Eye Clinical Examination - OSCE - Dr Gill
Direct Ophthalmoscopy use of the eyes is a very challenging clinical skill, incorporating both the examiner's knowledge of the retina, but also understanding the use of the ophthalmoscope
In this clinical skills tutorial, we look at the use of the direct ophthalmoscope as part of an ophthalmic examination
it should be noted that in the ideal circumstances, the room lights will be dimmed during the examination, and dilating eye drops used to improve the visualisation of the fundus
Some people may notice an ASMR effect from this clinical examination
#DrGill #Ophthalmoscopy #ClinicalSkills #EyeExam

In this animated episode of eOrthopodTV, orthopedic surgeon Randale C. Sechrest, MD narrates the procedure to replace an arthritic knee with an artificial joint.

Today I'm using the best 3D animation to explain WHAT IS DIASTASIS RECTI and what you need to know about diastasis recti after pregnancy! Grab the Complete Diastasis Recti Healing Guide: https://landing.mailerlite.com..../webforms/landing/n0
If you are't sure what video to start with and you just want step-by-step daily instructions you can start my 30-day core healing program. You get a new 10-min core healing video daily for 30 days. https://pregnancyandpostpartum....tv.thinkific.com/cou
How I healed my 4-finger diastasis recti gap:
Jessica Pumple is a registered dietitian, and pre & postnatal fitness instructor and certified pregnancy and postpartum core exercise specialist (CPES). She helps pregnant women stay fit, have healthy babies, and easier labors. She helps new moms with postpartum recovery, to heal and strengthen their core and feel energized after pregnancy!
If you enjoy our content subscribe to our channel, hit the bell button, leave a comment and share with your friends so I can make you more of the videos you enjoy!
Disclaimer: This is general postnatal fitness only. Please check with your doctor or health care provider to see if this video is safe for you. Wait until you get clearance (usually 4-6 weeks or 6-8 weeks after a c-section).You are responsible for your own safety. Don’t do anything that feels unsafe for you or baby. Stop if you have any pain or discomfort, bleeding, chest pain or shortness of breath, dizziness or if you feel unwell. P&P Health Inc., Pregnancy and Postpartum TV and Jessica Pumple are not liable in any way for any injury, loss, damages, costs or expenses suffered by you in relation to this video or its content.
Copyright 2023 P&P Health Inc. All rights reserved
#diastasisrecti #whatisdiastasisrecti #3danimation
Music: Epidemic Sound

Unique 3D technology from Olympus:
http://www.olympus-europa.com/....medical/en/medical_s
Discover the 3rd dimension of endoscopy and experience laparoscopy in a totally new dimension.
Contact us for more information:http://www.olympus-europa.com/....medical/en/medical_s

WARNING: Explicit and Educational Surgical Content.
Visage Clinic's Dr. Marc DuPéré - located in Toronto, Ontario, Canada discusses Liposuction (upper bra, back rolls, lower back rolls, love handles & abdomen) and "Tummy Tuck" (Abdominoplasty): Skin excision, muscle repair and umbilicoplasty.
For more info and to book a consultation visit www.VisageClinic.com/cosmetic-....surgery/mommy-makeov or call (416) 929-9800.

Do you think you have a hernia?
What are hernias?
The hernias we address in this http://DoctorsExpressHartsdale.com Medical Minute are inguinal, or groin, hernias. More common in men than women, an inguinal hernia can occur when part of the small intestine protrudes through a weakness or tear in the area between your abdomen and your thigh- or your groin. It's possible for anyone to get an inguinal hernia, but it is more commonly found in males.
Hernias form a bulge and can be accompanied by pain. Men have an approximate 26% lifetime risk of having hernia at some point in their life, where as women have a much lower chance of one- only about 3% of women will experience a hernia at some point in their life. There are other types of hernias, such as abdominal, or "hiatal" hernias but groin hernias outnumber abdominal hernias by about 3 to 1.
What causes a hernia?
The cause of a hernia is not always known, but hernias are often the result of weak spots in the abdominal wall. Weaknesses can be due to congenital defects (present at birth) or formed later in life. Some risk factors for inguinal hernia include:
• fluid or pressure in the abdomen
• heavy lifting
• straining during urination or bowel movements
• obesity
• chronic cough
• pregnancy
Hernias often form in people with weakened abdominal muscles or in those who do a lot of heavy lifting or straining, which is why we see it quite often in young men. Physiology plays a part: men have testicles and scrotum which descend through the inguinal canal-much larger in men than in women. That is part of the reason men tend to be more susceptible to hernias than women.
Symptoms of hernia
Symptoms of inguinal hernia usually include a bulge in the groin area and pain, pressure, or aching at the bulge—especially when lifting, bending, or coughing. These symptoms usually subside during rest periods. Men may also experience swelling around the testicles.
Screening and Diagnosis of Hernias
If you are having abdominal pain or pelvic bulge and pain, you want to see physician, and he or she will do an exam. They will use their finger, to see if you have a bulge in your scrotum or on your groin and they'll see if its reducible or not. If the exam doesn't give them the answer, they can then perform an ultrasound, an inexpensive test that can tell you the same day whether a hernia is present.
What to do if you think you have a hernia
Most of the time hernias do not cause problems. People often live with hernias their entire life without them becoming aggravated or painful. When they do cause pain though, there is concern that complications may have arisen. Most common hernias are what we call reducible; you can take your finger or you can lie down in bed and due to the effects of gravity, the bulge in the groin will actually disappear, which means the intestinal contents actually go back into the abdominal cavity or to the correct location. If it's not reducible by lying down or using a finger or having a physician trying to reduce it, then there are concerns about complications such as strangulation, or incarceration occurring. If those concerns are there, then you need to see a surgeon, and there may be a need for surgery.
How to Treat a Hernia
As stated earlier, hernias can often be watched for years without being treated. If however, they are causing pain, we generally refer you to a surgeon who can do a very simple laparoscopic surgery.
If you suspect a hernia, but have not been diagnosed, you should see your doctor, and of course, we are happy to see you here at Doctors Express


Thousands of Canadians undergo surgery every year, so how can you best prepare? The first step is having a dialogue, says Sunnybrook anesthesiologist Dr. Colin McCartney. Read the blog for more: http://sunnyview.sunnybrook.ca

If you are tired of dealing with glasses or squinting to read signs in the distance, then you should consider LASIK Eye Surgery. In this outpatient refractive procedure, lasers are used to correct vision issues by changing the structure of the cornea. This may entirely eliminate reliance upon glasses or contacts. In this interactive LASIK Eye Surgery, you will assist in numbing the patient’s eye and cleaning the area for the procedure. With a speculum, you will hold the eye open, mark the cornea using a water-soluble ink, then attach a suction ring to it. After that, a specialized blade device is used to cut into the corneal flap and peel it back so that the laser can clear away corneal tissue underneath. This process corrects the shape of the cornea in less than a minute before putting the corneal flap back in place. After the procedure, we will go over LASIK Eye Surgery recovery instructions. Scrub in and let’s get started!
