- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Middle cerebral artery syndrome is a condition whereby the blood supply from the middle cerebral artery (MCA) is restricted, leading to a reduction of the function of the portions of the brain supplied by that vessel: the lateral aspects of frontal, temporal and parietal lobes, the corona radiata, globus pallidus, caudate and putamen. The MCA is the most common site for the occurrence of ischemic stroke.[1] Depending upon the location and severity of the occlusion, signs and symptoms may vary within the population affected with MCA syndrome. More distal blockages tend to produce milder deficits due to more extensive branching of the artery and less ischemic response. In contrast, the most proximal occlusions result in widespread effects that can lead to significant cerebral edema, increased intracranial pressure, loss of consciousness and could even be fatal.[1] In such occasions, mannitol (osmotic diuretic) or hypertonic saline are given to draw fluid out of the oedematus cerebrum to minimise secondary injury. Hypertonic saline is better than mannitol, as mannitol being a diuretic will decrease the mean arterial pressure and since cerebral perfusion is mean arterial pressure minus intracranial pressure, mannitol will also cause a decrease in cerebral perfusion. Contralateral hemiparesis and hemisensory loss of the face, upper and lower extremities is the most common presentation of MCA syndrome.[1] Lower extremity function is more spared than that of the faciobrachial region.[2] The majority of the primary motor and somatosensory cortices are supplied by the MCA and the cortical homunculus can, therefore, be used to localize the defects more precisely.it is important to note that middle cerebral artery lesions mostly affect the dominant hemisphere i.e. the left cerebral hemisphere.
Kawasaki disease is a condition that causes inflammation in the walls of medium-sized arteries throughout the body, including the coronary arteries, which supply blood to the heart muscle. Kawasaki disease is also called mucocutaneous lymph node syndrome because it also affects lymph nodes, skin, and the mucous membranes inside the mouth, nose and throat. Signs of Kawasaki disease, such as a high fever and peeling skin, can be frightening. The good news is that Kawasaki disease is usually treatable, and most children recover from Kawasaki disease without serious problems.

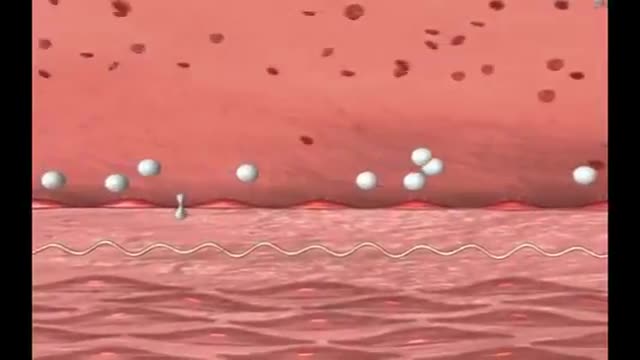
LDL (Bad) Cholesterol LDL cholesterol is considered the “bad” cholesterol because it contributes to plaque, a thick, hard deposit that can clog arteries and make them less flexible. This condition is known as atherosclerosis. If a clot forms and blocks a narrowed artery, heart attack or stroke can result. Another condition called peripheral artery disease can develop when plaque buildup narrows an artery supplying blood to the legs. View an animation of cholesterolHDL (Good) Cholesterol HDL cholesterol is considered “good” cholesterol because it helps remove LDL cholesterol from the arteries. Experts believe HDL acts as a scavenger, carrying LDL cholesterol away from the arteries and back to the liver, where it is broken down and passed from the body. One-fourth to one-third of blood cholesterol is carried by HDL. A healthy level of HDL cholesterol may also protect against heart attack and stroke, while low levels of HDL cholesterol have been shown to increase the risk of heart disease.

Medial medullary syndrome, also known as Dejerine syndrome, represents less than 1% of brainstem stroke syndromes. Thrombotic or embolic occlusion of small perforating branches from vertebral or proximal basilar artery supplying the medial aspect of medulla oblongata cause this rare syndrome. It is characterized by contralateral hemiplegia/hemiparesis as well as hemisensory loss with ipsilateral hypoglossal palsy (ipsilateral tongue weakness and atrophy) from involvement of CN XII nucleus. Other manifestations e.g. vertigo, nausea, ipsilateral limb ataxia are also reported.
Renal transplantation is the treatment of choice for a minority of patients with end-stage renal disease (ESRD). Most adult patients with ESRD are never referred for evaluation for transplantation, and have a 70% 5-year mortality on dialysis. Marked improvements in early graft survival and long-term graft function have made kidney transplantation a more cost-effective alternative to dialysis. In the United States, over 375,000 kidney transplants have been performed, and in 2012, 191,400 patients were alive and with a functioning transplanted kidney; currently, more than 101,000 patients are waiting for kidney transplants.[1, 2] Before the advent of immunosuppression, renal transplantation was limited to identical twins and was not applicable to the vast majority of patients with ESRD. The introduction of combined azathioprine-steroid therapy in 1963 produced encouraging results and became the mainstay of immunosuppression. Although this therapy improved the results of transplantation, acute rejection and complications associated with steroid therapy persisted. The introduction of cyclosporine in 1983 significantly improved the outcomes of all solid-organ transplants by reducing the risk of rejection. Further innovations, including anti–T cell antibodies (both monoclonal and polyclonal preparations), as well as other maintenance immunosuppressants (eg, tacrolimus, mycophenolate, sirolimus), have made a significant impact on both patient and graft survival. Currently, 1-year patient and graft survival rates exceed 90% in most transplant centers. For patient education information, see Kidney Transplant and the Mayo Clinic's kidney transplant information Web page.

Hepatitis is an inflammation of the liver. The condition can be self-limiting or can progress to fibrosis (scarring), cirrhosis or liver cancer. Hepatitis viruses are the most common cause of hepatitis in the world but other infections, toxic substances (e.g. alcohol, certain drugs), and autoimmune diseases can also cause hepatitis. There are 5 main hepatitis viruses, referred to as types A, B, C, D and E. These 5 types are of greatest concern because of the burden of illness and death they cause and the potential for outbreaks and epidemic spread. In particular, types B and C lead to chronic disease in hundreds of millions of people and, together, are the most common cause of liver cirrhosis and cancer. Hepatitis A and E are typically caused by ingestion of contaminated food or water. Hepatitis B, C and D usually occur as a result of parenteral contact with infected body fluids. Common modes of transmission for these viruses include receipt of contaminated blood or blood products, invasive medical procedures using contaminated equipment and for hepatitis B transmission from mother to baby at birth, from family member to child, and also by sexual contact. Acute infection may occur with limited or no symptoms, or may include symptoms such as jaundice (yellowing of the skin and eyes), dark urine, extreme fatigue, nausea, vomiting and abdominal pain.
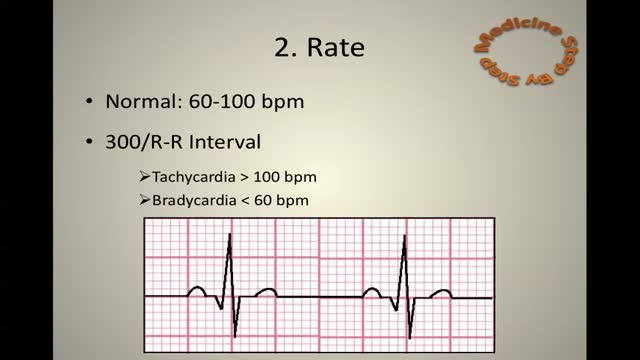
ECG Learn it
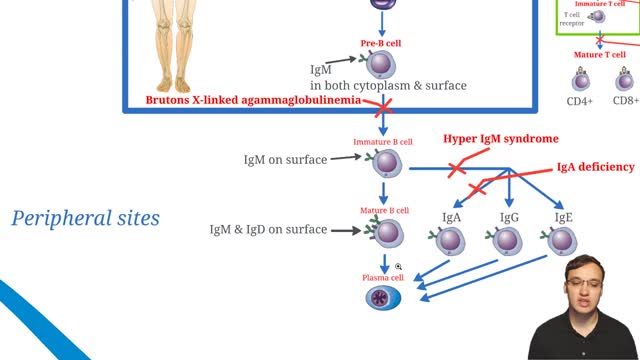
X-linked agammaglobulinemia (XLA), or Bruton agammaglobulinemia, is an inherited immunodeficiency disease caused by mutations in the gene coding for Bruton tyrosine kinase (BTK). The disease was first elucidated by Bruton in 1952, for whom the gene is named. BTK is critical to the maturation of pre–B cells to differentiating mature B cells. The BTK gene defect has been mapped to the long arm of the X chromosome at band Xq21.3 to Xq22, spanning 37.5kb with 19 exons forming 659 amino acids to complete the BTK cytosolic tyrosine kinase. A database of BTK mutations (BTKbase: Mutation registry for X-linked agammaglobulinemia) lists 544 mutation entries from 471 unrelated families showing 341 unique molecular events. No single mutation accounts for more than 3% of mutations in patients. In addition to mutations, a number of variants or polymorphisms have been found.
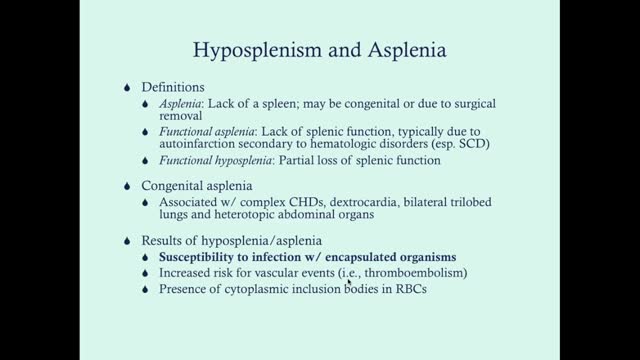
Asplenia is the absence of spleen and/or its functions. Abnormalities of the spleen may be classified on a pattern oriented approach, based on splenic imaging.[1] These include anomalies of the following: Shape (clefts, notches, lobules) Location (wandering spleen) Number (asplenia, polysplenia) Size (splenomegaly, atrophy) Solitary lesions (cysts, lymphangiomas, hemangiomas, hamartomas) Multiple lesions (trauma, infections, neoplasms, storage disorders) Diffuse disease (infarction, heavy metal deposition, peliosis) Absence of splenic tissue can be total (congenital asplenia) or partial (hypoplastic) from birth. Loss of splenic tissue due to surgical removal may occur later in life as a result of trauma that causes rupture of the organ. The spleen may be removed in other conditions (eg, hemoglobinopathies) to improve the red cell life expectancy. Removal of the spleen may be undertaken as a result of being involved in a neoplastic processor as a staging procedure in some cancers. Occasionally, the spleen may be removed to address the sheer mass effect of a massive enlargement (such as in storage disorders), which can cause mass effects. Autosplenectomy is the process where the spleen loses its function due to multiple and repeated infarctive episodes, as in sickle hemoglobinopathies. See the image below.
Friedreich's ataxia is an inherited disease that damages your nervous system. The damage affects your spinal cord and the nerves that control muscle movement in your arms and legs. Symptoms usually begin between the ages of 5 and 15. The main symptom is ataxia, which means trouble coordinating movements. Specific symptoms include Difficulty walking Muscle weakness Speech problems Involuntary eye movements Scoliosis (curving of the spine to one side) Heart palpitations, from the heart disease which can happen along with Friedreich's ataxia People with Friedreich's ataxia usually need a wheelchair 15 to 20 years after symptoms first appear. In severe cases, people become incapacitated. There is no cure. You can treat symptoms with medicines, braces, surgery, and physical therapy.
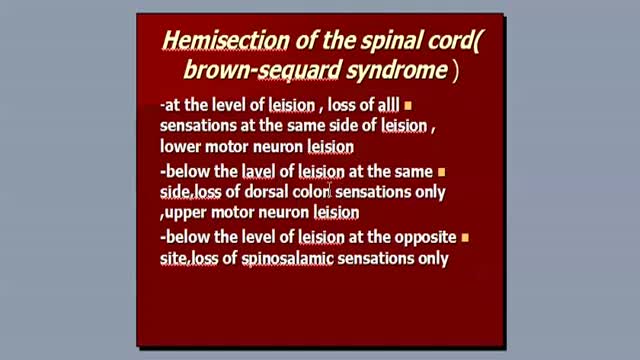
Brown-Séquard syndrome is an incomplete spinal cord lesion characterized by a clinical picture reflecting hemisection injury of the spinal cord, often in the cervical cord region. (See Presentation.) Patients with Brown-Séquard syndrome suffer from ipsilateral upper motor neuron paralysis and loss of proprioception, as well as contralateral loss of pain and temperature sensation. A zone of partial preservation or segmental ipsilateral lower motor neuron weakness and analgesia may be noted. Loss of ipsilateral autonomic function can result in Horner syndrome. (See Etiology, Presentation, and Workup.) As an incomplete spinal cord syndrome, the clinical presentation of Brown-Séquard syndrome may range from mild to severe neurologic deficit. (See Presentation.) Brown-Séquard–plus syndrome The pure Brown-Séquard syndrome reflecting hemisection of the cord is not often observed. A clinical picture composed of fragments of the syndrome or of the hemisection syndrome plus additional symptoms and signs is more common. These less-pure forms of the disorder are often referred to as Brown-Séquard–plus syndrome.[1] Interruption of the lateral corticospinal tracts, the lateral spinal thalamic tract, and at times the posterior columns produces a picture of a spastic, weak leg with brisk reflexes and a strong leg with loss of pain and temperature sensation. Note that spasticity and hyperactive reflexes may not be present with an acute lesion.
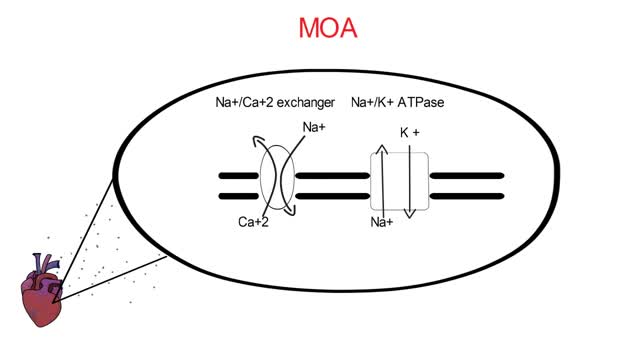
The incidence of digitalis toxicity has declined in recent years, due to decreased use of this drug along with improved technology for monitoring of drug levels and increased awareness of drug interactions. Nevertheless, cardiac glycoside toxicity continues to be a problem in the United States because of the wide use of digoxin (a preparation of digitalis) and its narrow therapeutic window. Digitalis is a plant-derived cardiac glycoside commonly used in the treatment of chronic heart failure (CHF), atrial fibrillation, and reentrant supraventricular tachycardia.[1, 2] Digoxin is the only available preparation of digitalis in the United States. (See Etiology and Epidemiology.) Cardiac glycosides are found in certain flowering plants, such as oleander and lily-of-the-valley. Indigenous people in various parts of the world have used many plant extracts containing cardiac glycosides as arrow and ordeal poisons. The ancient Egyptians used squill (Urginea maritime) as a medicine. The Romans employed it as a diuretic, heart tonic, emetic, and rat poison. Digitalis, or foxglove, was mentioned in the year 1250 in the writings of Welsh physicians. Fuchsius described it botanically 300 years later and named it Digitalis purpurea. William Withering published his classic account of foxglove and some of its medical uses in 1785, remarking upon his experience with digitalis. He recognized many of the signs of digitalis toxicity, noting, "The foxglove, when given in very large and quickly repeated doses, occasions sickness, vomiting, purging, giddiness, confused vision, objects appearing green or yellow; increased secretion of urine, slow pulses, even as low as 35 in a minute, cold sweats, convulsions, syncope, death." (See Presentation and Workup.) During the early 20th century, as a result of the work of Cushny, Mackenzie, Lewis, and others, the drug was gradually recognized as specific for treatment of atrial fibrillation. Only subsequently was the value of digitalis for treatment of CHF established. Cardiac glycosides enhance cardiac contractility and slow conduction through the atrioventricular (AV) junction by increasing vagal tone.[3] (See Etiology.) Cardiac glycoside toxicity has been known to result from ingestion of some plants, including yellow oleander (Thevetia peruviana) and foxglove, and a similar toxidrome has been associated with the use of herbal dietary supplements that contain cardiac glycosides. Digoxin is among the top 50 prescribed drugs in the United States.[4] In 2011, the American Association of Poison Control Centers reported 1601 single exposures to cardiac glycoside drugs.[5] Cardiac glycosides account for 2.6% of toxic plant exposures in the United States.[6, 7] Most of these exposures are in children.[7] (See Epidemiology.) Digoxin-specific fragment antigen-binding (Fab) antibody fragments have contributed significantly to the improved morbidity and mortality of toxic patients since their approval in 1986 by the US Food and Drug Administration (FDA). (See Prognosis, Treatment, and Medication.)
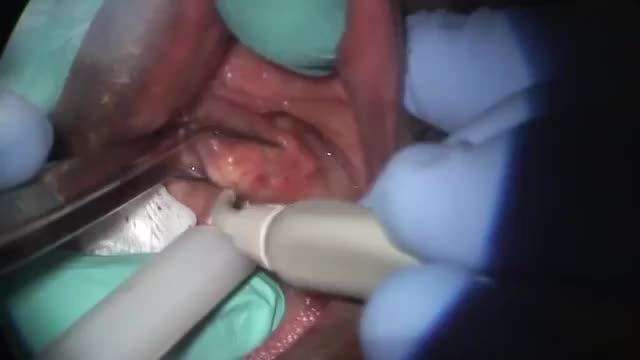
A salivary gland stone -- also called salivary duct stone -- is a calcified structure that may form inside a salivary gland or duct. It can block the flow of saliva into the mouth. The majority of stones affect the submandibular glands located at the floor of the mouth. Less commonly, the stones affect the parotid glands, located on the inside of the cheeks, or the sublingual glands, which are under the tongue. Many people with the condition have multiple stones. Salivary Gland Stone Causes and Symptoms Salivary stones form when chemicals in the saliva accumulate in the duct or gland. They mostly contain calcium. The exact cause is not known. But factors contributing to less saliva production and/or thickened saliva may be risk factors for salivary stones. These factors include: dehydration, poor eating, and use of certain medications (such as antihistamines), blood pressure drugs, psychiatric drugs, and bladder control drugs. Trauma to the salivary glands may also raise the risk for salivary stones. The stones cause no symptoms as they form, but if they reach a size that blocks the duct, saliva backs up into the gland, causing pain and swelling. You may feel the pain off and on, and it may get progressively worse. Inflammation and infection within the affected gland may follow. Salivary Gland Stones Diagnosis and Treatments If you have symptoms of a salivary gland stone, your doctor will first check for stones with a physical exam. Sometimes tests may also be ordered, such as X-ray, CT scan, or ultrasound.

Is My Chest Pain a Sign Of a Heart Attack?

The dog bite victim needs to be taken to a safe place away from the assailant dog to prevent further attack and injury. Since dog bites can cause significant damage beneath the skin, a type of injury that cannot always easily be appreciated, medical care should be accessed by a health care practitioner. Wounds should be kept elevated and, if possible, washing the wound with tap water may be attempted. Information should be obtained from the dog's owner about the dog's rabies immunization status, but if this is not possible, hospital, animal control centers, or law enforcement personnel will help gather any required information.

How to Treat Cuts & Scrapes | First Aid Training
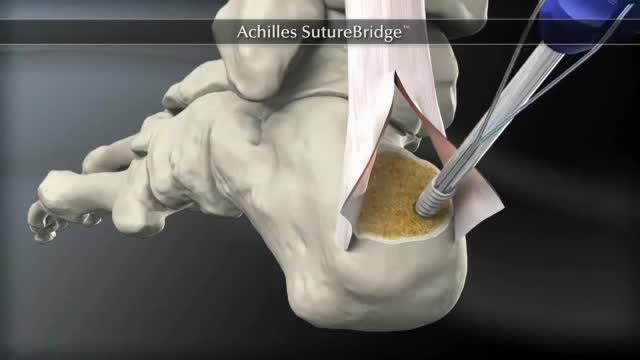
The Arthrex SpeedBridge™ is an innovative soft tissue fixation device used in the treatment of Achilles injuries. While standard anchor fixation of the tendon creates only a single point of compression directly over the anchor, the SpeedBridge enables an hourglass pattern of FiberTape® suture to be laid over the distal end of the tendon. This four-anchor construct enables a true knotless repair and a greater area of compression for the Achilles tendon on the calcaneus, improving stability and possibly allowing for earlier return to normal activities.
Colorectal cancer screening tests Screening is the process of looking for cancer in people who have no symptoms of the disease. Several tests can be used to screen for colorectal cancers. These tests can be divided into: Tests that can find both colorectal polyps and cancer: These tests look at the structure of the colon itself to find any abnormal areas. This is done either with a scope put into the rectum or with special imaging (x-ray) tests. Polyps found during these tests can be removed before they become cancerous, so these tests may prevent colorectal cancer. Because of this, these tests are preferred if they are available and you are willing to have them. Tests that mainly find cancer: These tests check the stool (feces) for signs of cancer. These tests are less invasive and easier to have done, but they are less likely to detect polyps.
Coronary artery bypass graft surgery (CABG) is a procedure used to treat coronary artery disease. Coronary artery disease (CAD) is the narrowing of the coronary arteries – the blood vessels that supply oxygen and nutrients to the heart muscle. CAD is caused by a build-up of fatty material within the walls of the arteries. This build-up narrows the inside of the arteries, limiting the supply of oxygen-rich blood to the heart muscle. One way to treat the blocked or narrowed arteries is to bypass the blocked portion of the coronary artery with a piece of a healthy blood vessel from elsewhere in the body. Blood vessels, or grafts, used for the bypass procedure may be pieces of a vein from the legs or an artery in the chest. An artery from the wrist may also be used. One end of the graft is attached above the blockage and the other end is attached below the blockage. Blood is routed around, or bypasses, the blockage by going through the new graft to reach the heart muscle. This is called coronary artery bypass surgery. Traditionally, to bypass the blocked coronary artery, a large incision is made in the chest and the heart is temporarily stopped so that the surgeon can perform the delicate procedure. To open the chest, the breastbone (sternum) is cut in half and spread apart. Once the heart is exposed, tubes are inserted into the heart so that the blood can be pumped through the body by a cardiopulmonary bypass machine (heart-lung machine). The bypass machine is necessary to pump blood while the heart is stopped and kept still in order for the surgeon to perform the bypass operation. While the traditional "open heart" procedure is still commonly done and often preferred in many situations, less invasive techniques have been developed to bypass blocked coronary arteries. "Off-pump" procedures, in which the heart does not have to be stopped, were developed in the 1990's. Other minimally invasive procedures, such as keyhole surgery (performed through very small incisions) and robotic procedures (performed with the aid of a moving mechanical device), may be used.

http://123-paleo.info-pro.co Gesunde Ernährung, Ernährung Umstellen, Marcumar Ernährung, Paleo Lebensmittel, Paleo Rezept. Wahrscheinlich wirst du dich als Paleo-Anhänger schon einmal gefragt haben, warum die Steinzeiternährung Getreide meidet wie die Pest. Gut, die Begründung, dass Menschen vor Tausenden von Jahren ebenfalls kein Getreide hatten, ist ja schön. Aber das kann ja nicht alles sein. Ist es auch nicht. Wie immer liegt der Teufel im Detail. Hauptverantwortlich für die große „Angst“ vor Getreideprodukten sind vor allem Gluten, sogenannte Anti-Nährstoffe. Bereits dieser Name ist angsteinflößend. Und das durchaus zu Recht. Denn Gluten besitzen nur wenige positive, dafür jedoch umso mehr negative Eigenschaften, die sich längerfristig schlecht auf deine Gesundheit auswirken können. Was ist Gluten und welche Lebensmittel enthalten Gluten? Gluten ist ein Eiweiß mit besonders starken Klebeeigenschaften. Dies ist auch der Grund, weswegen beispielsweise Brotteig so gut zusammenklebt. Gluten findet sich hauptsächlich in Getreide, beispielsweise ein Roggen oder Gerste, Dinkel oder Weizen und Hafer. Hieraus ergibt sich zwangsläufig, dass auch viele Lebensmittel des täglichen Lebens jede Menge Gluten enthalten. Hierzu gehören nicht nur Schokolade oder Bier, Reis oder Nudeln, sondern auch Pommes oder Milcherzeugnisse. Auch in den meisten Fertiggerichten ist Gluten vorzufinden.
