- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Wow! Ultrasound guided internal jugular vein cannulation (long axis approach)

Amazing Lung Inflation
Lip augmentation is a cosmetic procedure that can give you fuller, sensual, plumper lips that are now considered aesthetically appealing. Dr. Ajaya Kashyap best cosmetic & plastic surgeon in Delhi at MedSpa Clinic. Learn more about #lipaugmentation at www.bestfacesurgeryindia.com Learn more about #lipenhancement at www.themedspa.us/cosmetic-surgery/lip-enhancement.html Contact us : info@themedspa.us http://www.themedspa.us/contact.html Tag: lipaugmentation, lipenhancement, fullerlips, lipenlargement, lipfullness, nonsurgicalprocedure, fillers, cosmeticsurgery, dermalfiller, plumperlips, lipinjections, plumplips, injectablefillers, lipimplant, lip augmenation cost in delhi, lip augmenation in delhi , lip augmenation cost in India, best lip augmenation cost in delhi
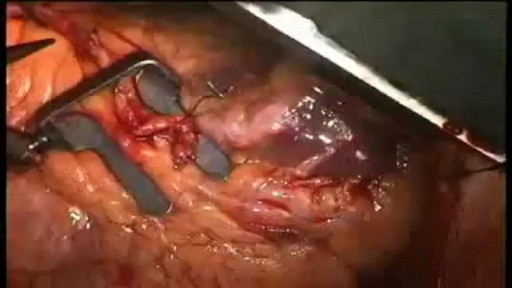
When your arteries cannot supply enough blood to your heart, your doctor may recommend coronary artery bypass graft (CABG) surgery. One of the most common heart surgeries in the United States, CABG surgery restores blood flow to your heart. Approximately every 10 minutes, someone has beating heart or "off-pump" bypass surgery1. Beating heart bypass surgery is — in simple terms — bypass surgery that is performed on your heart while it is beating. Your heart will not be stopped during surgery. You will not need a heart-lung machine. Your heart and lungs will continue to perform during your surgery. Surgeons use a tissue stabilization system to immobilize the area of the heart where they need to work. Beating heart bypass surgery is also called Off Pump Coronary Artery Bypass Surgery (OPCAB). Both OPCAB and conventional on-pump surgery restore blood flow to the heart. However, off-pump bypass surgery has proven to reduce side effects in certain types of patients.
In caring for patients who are critically ill, access to the central venous circulation is important. Central venous access allows the placement of various types of intravenous (IV) lines to facilitate the infusion of fluids, blood products, and drugs and to obtain blood for laboratory analysis. It is also an essential procedure in patients in whom placement of a line in a peripheral vein is impossible. A central line may be the only means of venous access in such cases.

Posterior dislocations with associated fractures, also known as complex posterior dislocations, often require open reduction and fixation (ORIF). These dislocations are often associated with significant ligamentous injury. In some cases, complex posterior elbow dislocations may be managed with closed reduction. Posterior elbow dislocations that are neglected, as is not uncommon in developing countries, can often be effectively treated with open reduction. [9] Delayed vascular compromise is an important complication after reduction. All patients should be observed for a period of approximately 2-3 hours after reduction. If no evidence of vascular compromise arises, patients can be sent home with appropriate follow-up and instructions to watch for further problems.

Bipolar disorder, formerly called manic depression, is a mental health condition that causes extreme mood swings that include emotional highs (mania or hypomania) and lows (depression). When you become depressed, you may feel sad or hopeless and lose interest or pleasure in most activities. When your mood shifts to mania or hypomania (less extreme than mania), you may feel euphoric, full of energy or unusually irritable. These mood swings can affect sleep, energy, activity, judgment, behavior and the ability to think clearly. Episodes of mood swings may occur rarely or multiple times a year. While most people will experience some emotional symptoms between episodes, some may not experience any. Although bipolar disorder is a lifelong condition, you can manage your mood swings and other symptoms by following a treatment plan. In most cases, bipolar disorder is treated with medications and psychological counseling (psychotherapy).

Scientists Create Artificial Womb

Baby massage for constipation relieving.

Every year, thousands of conventional total shoulder replacements are successfully done in the United States for patients with shoulder arthritis. This type of surgery, however, is not as beneficial for patients with large rotator cuff tears who have developed a complex type of shoulder arthritis called "cuff tear arthropathy." For these patients, conventional total shoulder replacement may result in pain and limited motion, and reverse total shoulder replacement is a better option.

First aid steps to help stop or shorten a seizure or prevent an emergency situation. This may involve giving a rescue treatment (often called "as needed" medicine or treatment) that has been recommended by your health care team. The rescue treatments described here can be given by non-medical people who are not in a hospital setting. They are intended for use by anyone (the person with seizures, family member or other observer) who has been trained in their use. These therapies can be given anywhere in the community

Hardware removals are among the most commonly performed surgical procedures worldwide. Current literature offers little data concerning postoperative patient satisfaction. The purpose of our study was to evaluate the patients’ point of view on implant removal. watch to learn more.
Human Circulatory System and heart video
This process involves surgical removing of an #organ or tissue from one person (organ donor) & placing into another person (recipient) body. https://goo.gl/JfoN8y
How to use a Syphilis rapid test kit for self-diagnosis of Syphilis (fingerstick blood). Convenient, Easy to Use, and over 99% Accurate. Certified GMP and ISO13485. Test yourself at home with Complete Privacy. Buy online today at: http://www.stdrapidtest.com
Real Story: Youngest Mother In History (5 years old) Pregnant FIVE YEAR OLD! Youngest Mother In The World, Lina Medina's True Story!

Spontaneous pneumothorax is a life-threatening condition in patients with severe underlying lung disease; thus, tube thoracostomy is the procedure of choice in SSP. Pleurodesis decreases the risk of recurrence, as does thoracotomy or video-assisted thoracoscopic surgery (VATS) to excise the bullae

The clinician performing the procedure should be familiar with the anatomy of the specific joint and cognizant of the relevant landmarks in order to avoid puncture of tendons, blood vessels, and nerves (see the images below).

A pacemaker insertion is the implantation of a small electronic device that is usually placed in the chest (just below the collarbone) to help regulate slow electrical problems with the heart.
Transvenous cardiac pacing, also called endocardial pacing, is a potentially life saving intervention used primarily to correct profound bradycardia. It can be used to treat symptomatic bradycardias that do not respond to transcutaneous pacing or to drug therapy.
