- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
They are the leaders of the pack when it comes to minimally invasive surgeries. Laparoscopic and robotic. Different techniques with the same benefits.
"There's significantly less blood loss, it's a quicker procedure, quicker recovery, less scarring, less chance for post operative wound complications or infections," says Dr. Darren Miter, laparoscopic surgeon with Lee Memorial Health System.
In a laparoscopic procedure surgeons operate through a series of poke holes, manually inserting thin cutting tools and a camera to provide magnified vision. It's used in a variety of surgical specialties.
"The vast majority of gallbladder surgeries are performed laparoscopically. A single incision in the belly button, one up under the breastbone and either one or two in the right upper side of the belly. Using long skinny instruments and looking up at a TV monitor, remove the gallbladder that way," says Dr. Miter.
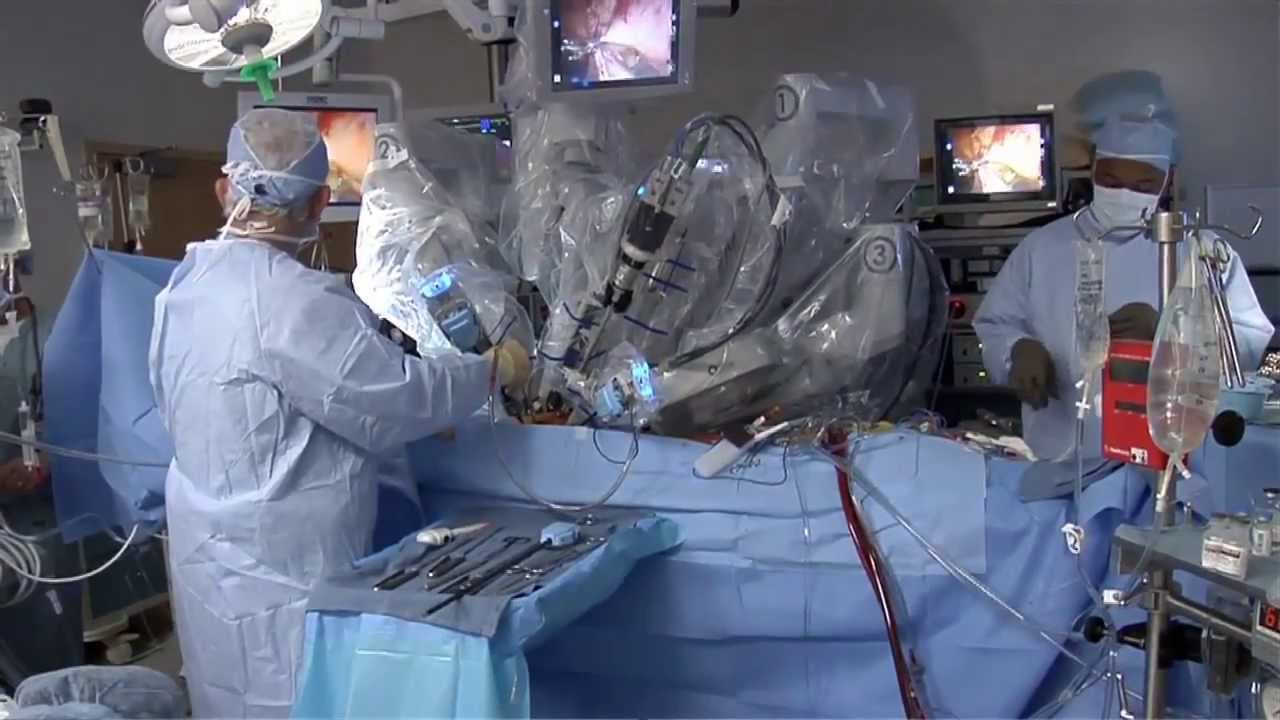
While laparoscopic is a hands-on approach, robotic procedures are surgeon-controlled. Working at a console, surgeons direct the robotic arms, which have super-human capabilities and 3D, hi def vision.
"I mean you have to see it to believe it, that's a great tool to have. You got a very good depth perception. Plus the other thing when you're working with your hands it's more intuitive," says Dr. Nagesh Ravipati, colorectal surgeon with Lee Memorial Health System.
The robotic system performs maneuvers the human hand can't.
"Especially if you have to do any suturing, it is so much simpler with the robots because you can just turn around 360 degrees," says Dr. Ravipati.
Robotic surgery is gaining momentum in precise procedures, including the field of cancer.
"The robot is good when you're going to operate on just one field. For rectal surgery you're in one place, it's docked. It gives you the best 3 dimensional vision," says Dr. Ravipati.
Robotic and laparoscopic. Both cutting edge options, with less cutting.
View More Health Matters video segments at leememorial.org/healthmatters/
Lee Memorial Health System in Fort Myers, FL is the largest network of medical care facilities in Southwest Florida and is highly respected for its expertise, innovation and quality of care. For nearly a century, we've been providing our community with everything from primary care treatment to highly specialized care services and robotic assisted surgeries.
Visit leememorial.org

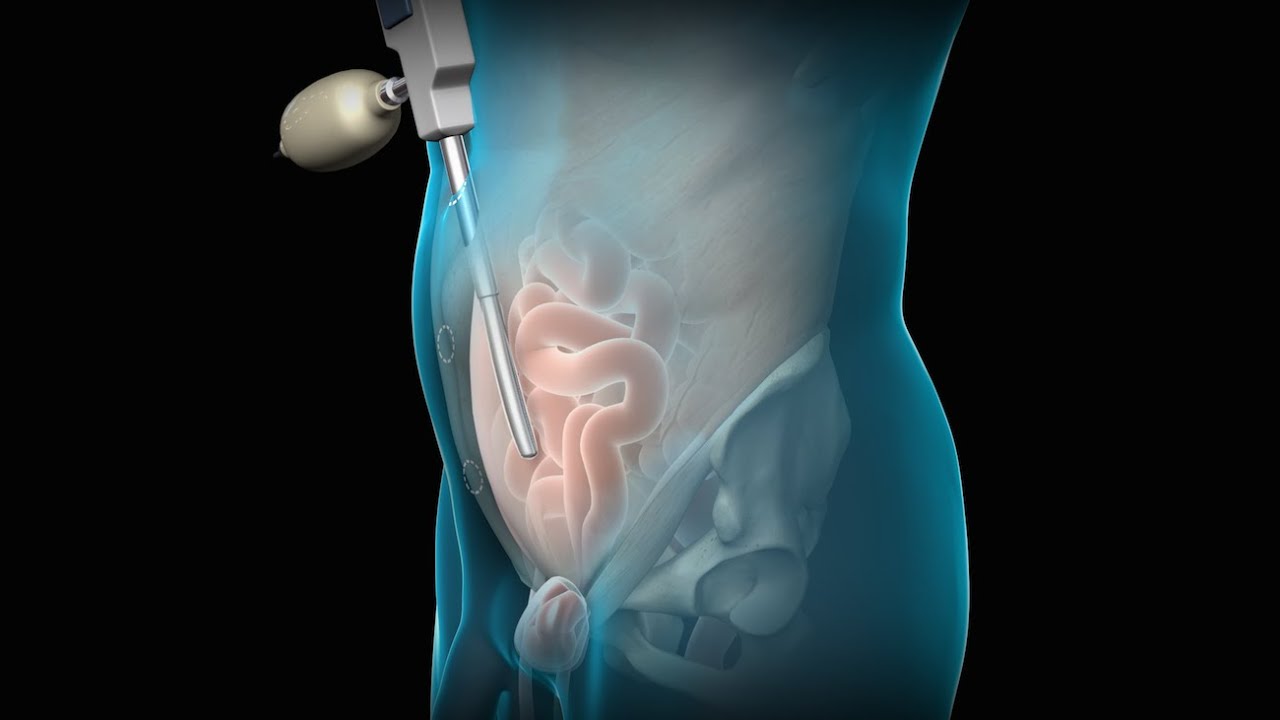
UChicago Medicine organ transplant surgeon Dr. Rolf Barth explains a how the laparoscopic donor nephrectomy – also known as the single-port nephrectomy – procedure works to remove an organ donor’s kidney from their body to be transplanted into a recipient. This minimally invasive kidney donor transplant surgery allows living organ donors the get back to their lives more quickly than the traditional approach and leaves them with a nearly invisible scar in the belly button.
Learn more about living kidney donation: https://www.uchicagomedicine.o....rg/conditions-servic
To license this video for patient education or content marketing, visit: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=tephernia-030615
An inguinal hernia is a bulging of the intestine through a defect or weak spot in the wall of the lower abdomen. This video shows how inguinal hernias form and how they are treated.
#TotalExtraperitonealLaparoscopicInguinalHerniaRepair #TEP #laparoscopy
ANCE00200
This medical animation shows laparoscopically assisted gallbladder removal surgery, or cholecystectomy. The animation begins by showing the normal anatomy of the liver and gallbladder. Over time, gallstones form within the gallbladder, blocking the cystic duct, and causing the gallbladder to become enlarged and inflamed. The procedure, sometimes called a "lap-chole", begins with the insertion of four trocar devices, which allow the physician to see inside the abdomen without making a large incision. Air is added to the abdominal cavity to make it easier to see the gall bladder. Next, we see a view through the laparascope, showing two surgical instruments grasping the gallbladder while a third severs the cystic duct. After the gallbladder is removed, the camera pans around to show that the cystic artery and vein, have already been clipped to prevent bleeding.
Item #ANIM026

This surgical animation is for patient education and describes a laparoscopic colectomy, which is a type of minimally invasive surgery for colon cancer. Laparoscopic colectomy, also called minimally invasive colectomy, involves several small incisions in your abdomen. Instead of a big incision, the surgeon makes a few small cuts (0.5-1 centimeters) in the abdominal cavity to insert a surgical camera and instruments and perform the operation. A slightly bigger incision, about 3.5 centimeters wide, is made to remove the tumor.
When compared to traditional open surgery, laparoscopic colectomy can result in much less pain and swifter recovery. Depending on the procedure, most laparoscopic colectomy patients leave the hospital and return to normal activities more quickly than patients recovering from open surgery.
Colorectal cancer is the second leading cause of cancer death in the United States.
For more information about 3d animation videos, please visit https://www.amerra.com

UPDATE 2/6/15: A new version of this animation is now available! https://www.youtube.com/watch?v=E1ljClS0DhM
This 3D medical animation depicts the surgical removal of the appendix (appendectomy) using laparoscopic instruments. The surgery animation begins by showing an inflamed appendix (appendicitis), followed by the placement of the laparoscope. Afterward, one can see the surgical device staple, cut and remove the inflamed appendix. Following the removal of the appendix the abdomen is flushed with a sterile saline solution to ensure all traces of infection have been removed.
ANCE00183

This video demonstrate Laparoscopic Cholecystectomy Full Length Skin to Skin Video with Infrared Cholangiography performed by Dr R K Mishra at World Laparoscopy Hospital. Infrared Cholegiography is performed by using Indocyanine Green during laparoscopic cholecystectomy surgery for gallbladder removal. Bile duct injury remains the most feared complication of laparoscopic cholecystectomy. Intraoperative cholangiography (IOC) is the current gold standard for biliary imaging and may reduce injury, but is not widely used because of the difficulties of doing it. Near-Infrared Fluorescence Cholangiography (NIRF-C) is a novel non-invasive method for real-time, radiation-free, intra-operative biliary mapping during laparoscopic cholecystectomy. We have experienced that NIRF-C is a safe and effective method for identifying biliary anatomy during laparoscopic cholecystectomy. Indocyanine green is a cyanine dye is very popular and used for many years in medical diagnostics. It is used for determining cardiac output, hepatic function, liver, and gastric blood flow, and for ophthalmic angiography. Now the use of this dye in lap chole has improved the safety of this surgery by NEAR INFRARED FLUORESCENT CHOLANGIOGRAPHY.
For more information please contact:
World Laparoscopy Hospital
Cyber City, Gurugram, NCR DELHI
INDIA 122002
Phone & WhatsApp: +919811416838, + 91 9999677788

Product demonstration video for the Cardinal Health™ Laparoscopic Abdominal Drape (cat. no. 9438)

This video demonstrates Laparoscopic Cholecystectomy Fully Explained Skin-to-Skin Video with Near Infrared Cholangiography performed by Dr R K Mishra at World Laparoscopy Hospital. A laparoscopic cholecystectomy is a minimally invasive surgical procedure that involves removing the gallbladder. It is typically performed using small incisions in the abdomen, through which a laparoscope (a thin tube with a camera and light) and surgical instruments are inserted. The surgeon uses the laparoscope to visualize the inside of the abdomen and to guide the instruments in removing the gallbladder.
Near-infrared cholangiography is a technique that uses a special camera and fluorescent dye to visualize the bile ducts during surgery. The dye is injected into the cystic duct (the tube that connects the gallbladder to the bile ducts) and the camera detects the fluorescence emitted by the dye, allowing the surgeon to see the bile ducts more clearly.
The combination of laparoscopic cholecystectomy and near-infrared cholangiography has become a standard of care in many hospitals and surgical centers. It allows for a more precise and efficient surgery, reducing the risk of complications such as bile duct injury.
The use of indocyanine green (ICG) with near-infrared imaging during laparoscopic cholecystectomy has several advantages. Here are some of them:
Better visualization of the biliary anatomy: ICG with near-infrared imaging allows for better visualization of the biliary anatomy during surgery. This helps the surgeon identify important structures, such as the cystic duct and the common bile duct, and avoid injuring them.
Reduced risk of bile duct injury: With better visualization of the biliary anatomy, the risk of bile duct injury during surgery is reduced. Bile duct injury is a serious complication that can occur during laparoscopic cholecystectomy and can lead to long-term health problems.
Improved surgical precision: ICG with near-infrared imaging also improves surgical precision. The surgeon can better see the tissues and structures being operated on, which can help reduce the risk of bleeding and other complications.
Shorter operating time: The use of ICG with near-infrared imaging can shorten the operating time for laparoscopic cholecystectomy. This is because the surgeon can more quickly and accurately identify the biliary anatomy, which can help streamline the surgery.
Overall, the use of ICG with near-infrared imaging is a valuable tool in laparoscopic cholecystectomy that can improve surgical outcomes and reduce the risk of complications.
Like any surgical procedure, laparoscopic cholecystectomy (gallbladder removal) has potential complications. Here are some of the most common ones:
Bleeding: Bleeding during or after the surgery is a possible complication of laparoscopic cholecystectomy. Most cases are minor and can be easily controlled, but in rare cases, significant bleeding may require a blood transfusion or even additional surgery.
Infection: Any surgical procedure carries a risk of infection. After laparoscopic cholecystectomy, there is a risk of infection at the site of the incisions or within the abdomen. Symptoms may include fever, pain, redness, or drainage from the incision sites.
Bile leakage: In some cases, a small amount of bile may leak from the bile ducts into the abdominal cavity after gallbladder removal. This can cause abdominal pain, fever, and sometimes requires further surgery or treatment.
Injury to nearby organs: During the surgery, there is a small risk of unintentional injury to nearby organs such as the liver, intestines, or bile ducts. This can cause additional complications and may require further treatment.
Adverse reactions to anesthesia: As with any surgery requiring general anesthesia, there is a small risk of adverse reactions to the anesthesia, such as an allergic reaction, respiratory problems, or heart complications.
Most patients recover without complications following a laparoscopic cholecystectomy, but it is important to discuss any concerns or questions with your surgeon beforehand.
Contact us
World Laparoscopy Hospital
Cyber City, Gurugram, NCR Delhi
INDIA : +919811416838
World Laparoscopy Training Institute
Bld.No: 27, DHCC, Dubai
UAE : +971525857874
World Laparoscopy Training Institute
8320 Inv Dr, Tallahassee, Florida
USA : +1 321 250 7653
Regenerate response


UPMC liver surgeons are among the most experienced in the world in performing minimally invasive liver surgery. Most patients benefit from less trauma and pain, minimal scarring, a shorter hospital stay, and faster recovery than from traditional surgery.
To learn more, please visit https://www.upmc.com/services/....liver-cancer/treatme

Dr. Erica Hodgman discusses pediatric surgery at the Johns Hopkins Children's Center Pediatric General Surgery program, what common surgeries the program specializes in, what makes the program unique and her work as a pediatric surgeon. #PediatricSurgery #JohnsHopkinsChildrenCenter
Questions Answered:
0:03 Describe the pediatric general surgery division at Johns Hopkins Children's Center.
1:00 What makes this program unique?
1:31 What are some common pediatric surgery cases?
2:23 Explain your work as a pediatric general surgeon?

Our surgeons take a compassionate, family-centered approach to both inpatient and outpatient care. We’re committed to making sure both you and your child understand our process. Told through a kid's eyes, this video tour reveals our caring approach.
To learn more about pediatric surgery at Stamford Hospital, visit: https://www.stamfordhealth.org..../care-treatment/pedi

When your child needs surgery, it can be overwhelming and sometimes scary. At Mayo Clinic Children’s Center, our highly skilled surgeons apply deep experience and specialized training to offer individualized care for your child and your family.

What to expect during the day of a pediatric surgery at Sutter Children's Center Sacramento.


World-renowned surgeons at Shriners Hospitals for Children – Northern California provide complex pediatric surgery for children one-year and older with congenital and acquired conditions. Children from throughout the Western United States with chest wall malformations, gastro-intestinal disease, ano-rectal disorders, urologic conditions and other complex surgical needs benefit from the expert care. The pediatric surgery team is devoted to the development of innovative and minimally invasive surgical techniques.
Johns Hopkins Children’s Center Surgeon-in-Chief David Hackam provides information about general pediatric surgery and when it is time to see a general pediatric surgeon. #PediatricSurgery #JohnsHopkins
For more information on general pediatric surgery at Johns Hopkins Children's Center, visit https://www.hopkinsmedicine.or....g/johns-hopkins-chil
FAQ's
0:02 What is a general pediatric surgeon?
0:31 When is it time to see a pediatric surgeon?
1:02 What are some of the most common surgical problems seen by general pediatric surgeons?
1:43 Describe research being done in the field.
2:15 Why choose Johns Hopkins Children's Center for general pediatric surgery?

Mr Brian MacCormack talking about Paediatric Surgery Emergencies. This talk is part of the Paediatric Emergencies 2022 event. To get your CME certificate for watching the video please visit https://www.paediatricemergenc....ies.com/conference/p
#PaediatricEmergencies #PaediatricEmergencies2022 #PaediatricSurgery

Children are special patients, and their medical needs are unique, including their surgical needs. At UNC Hospitals, an expert and experienced team of physicians treat children in a kid-friendly and family-centered environment. UNC Pediatric Surgeon Dr. Timothy Weiner explains
