- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Craniopharyngioma Complete Excision
Scientifically Erectile Dysfunction Penile Implants


In this video, we show a sports hernia self treatment we give many of our clients. It is not the only part of treatment. Grabbing the skin around the region of the groin strain can reduce pain and stiffness with turning and twisting. Sports hernias are often misdiagnosed with hip labrum tears, hip impingement, adductor tendonitis and abdominal strains.
Want more information? We have a more detailed free webinar on our page here. https://bit.ly/37thtNF
Want some treatment or suggestions of exercises or stretches? Contact us! We have in-person and virtual sessions.
Costa Mesa CA 715-502-4243 www.p2sportscare.com
Sports Hernia Diagnosis
What Is A Sports Hernia?
A sports hernia is tearing of the transversalis fascia of the lower abdominal or groin region. A common misconception is that a sports hernia is the same as a traditional hernia. The mechanism of injury is rapid twisting and change of direction within sports, such as football, basketball, soccer and hockey.
The term “sports hernia” is becoming mainstream with more professional athletes being diagnosed. The following are just to name a few:
Torii Hunter
Tom Brady
Ryan Getzlaf
Julio Jones
Jeremy Shockey
If you follow any of these professional athletes, they all seem to have the same thing in common: Lingering groin pain. If you play fantasy sports, this is a major headache since it seems so minor, but it can land a player on Injury Reserve on a moments notice. In real life, it is a very frustrating condition to say the least. It is hard to pin point, goes away with rest and comes back after activity, but is hardly painful enough to make you want to stop. It lingers and is always on your mind. And if you’re looking for my step-by-step sports hernia rehab video course here it is.
One the best definitions of Sport hernias is the following by Harmon:
The phenomena of chronic activity–related groin pain that it is unresponsive to conservative therapy and significantly improves with surgical repair.”
This is truly how sports hernias behave in a clinical setting. It is not uncommon for a sports hernia to be unrecognized for months and even years. Unlike your typical sports injury, most sports medicine offices have only seen a handful of cases. It’s just not on most doctors’ radar. The purpose of this article is not only to bring awareness about sports hernias, but also to educate.
Will you find quick fixes in this article for sports hernia rehab?
Nope. There is no quick fix for this condition, and if someone is trying to sell you one, they are blowing smoke up your you-know-what.
Is there a way to decrease the pain related to sports hernias?
Yes. Proper rehab and avoidance of activity for a certain period of time will assist greatly, but this will not always stop it from coming back. Pain is the first thing to go and last thing to come. Do not be fooled when you become pain-free by resting it. Pain is only one measure of improvement in your rehab. Strength, change of direction, balance and power (just to name a few) are important, since you obviously desire to play your sport again. If you wanted to be a couch potato, you would be feeling better in no time. Watching Sports Center doesn’t require any movement.
Why is this article so long?
There is a lot of information on sports hernias available to you on the web. However, much of the information is spread out all over the internet and hard for athletes to digest due to complicated terminology. This article lays out the foundational terminology you will need to understand what options you have with your injury. We will go over anatomy, biomechanics, rehab, surgery, and even the fun facts. The information I am using is from the last ten years of medical research, up until 2016. We will be making updates overtime when something new is found as well. So link to this page and share with friends. This is the best source for information on sports hernias you will find.
Common Names (or Aliases?) for Sports Hernias
Sportsman’s Hernia
Athletic Pubalgia
Gilmore’s Groin
How Do You Know If You Have A Sports Hernia?
Typical athlete characteristics:
Male, age mid-20s
Common sports: soccer, hockey, tennis, football, field hockey
Motions involved: cutting, pivoting, kicking and sharp turns
Gradual onset
How A Sports Hernia Develops
Chronic groin pain typically happens over time, which is why with sports hernias, we do not hear many stories of feeling a “pop” or a specific moment of injury. It is the result of “overuse” mechanics stemming from a combination of inadequate strength and endurance, lack of dynamic control, movement pattern abnormalities, and discoordination of motion in the groin area.
#sportsherniadiagnosisselftreatment #sportshernia #california

Ligation of Aneurysm in ArterioVenous Malformation

Eye Lid Partial Tarsectomy Surgery

Watch that video of The Biggest Ingrown Hair Removed
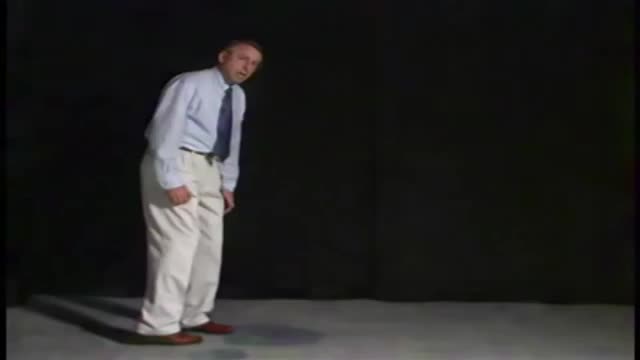
The patient has spasticity in the lower extremities greater than the upper extremities. The hips and knees are flexed and adducted with the ankles extended and internally rotated. When the patient walks both lower extremities are circumducted and the upper extremities are held in a mid or low guard position. This type of gait is usually seen with bilateral periventricular lesions. The legs are more affected than the arms because the corticospinal tract axons that are going to the legs are closest to the ventricles.
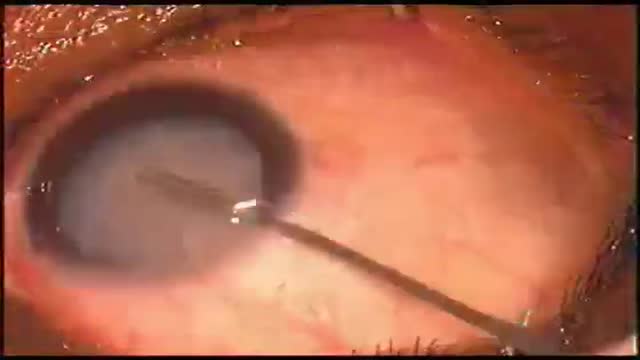
Eye Phacoemulsification
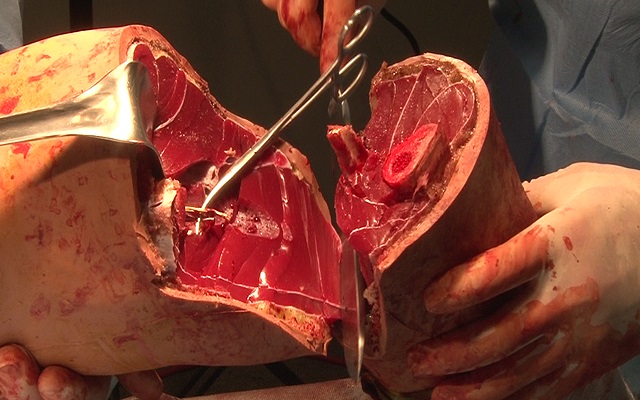
Watch that Above Knee Amputation Surgery video
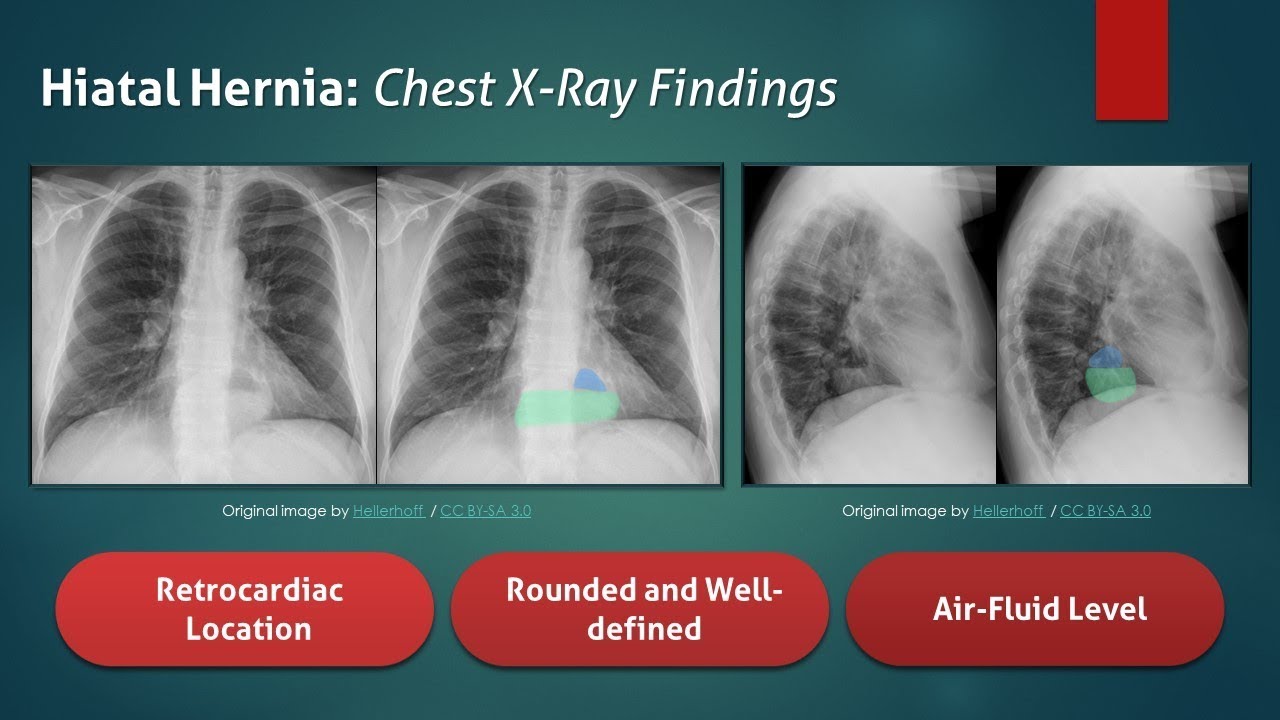
The typical radiograph is of a well-defined, rounded, retrocardiac opacity with an air-fluid level. In this image, the radiolucent gas is highlighted in blue, while the gastric contents are highlighted in the green. In many cases of hiatal hernia, there will not be an air bubble below the left hemidiaphragm. This is a relatively expected finding considering that the stomach is no longer in its usual position. The anatomical position of the herniated organ can be further elucidated on the lateral radiograph. Here we can see that the stomach is in the middle mediastinum posterior to the heart and above the diaphragm. Hiatal hernias can look similar to a retrocardiac lung abscess or another cavitary lesion, but it will change in size and shape between radiographs. Large hernias can shift the mediastinum to the right and result in a widening of the carinal angle. They can even give the appearance of cardiomegaly. In this radiograph, the cardiac silhouette is distinctly visible within the confines of the hiatal hernia. To review, a hiatal hernia on an AP chest radiograph typically appears as a round retrocardiac opacity with an air-fluid level.
🌐 Check out our website for more video lectures
https://www.med4vl.com
📺 Subscribe To My Channel and Get More Great Quizzes and Tutorials
https://www.youtube.com/channe....l/UC95TzSH1B_2EjaZMg
#FOAMrad #MedEd #radiology
Disclaimer: All the information provided by Medical Education for Visual Learners and associated videos are strictly for informational purposes only. It is not intended as a substitute for medical advice from your health care provider or physician. It should not be used to overrule the advice of a qualified healthcare provider, nor to provide advice for emergency medical treatment. If you think that you or someone that you know may be suffering from a medical condition, then please consult your physician or seek immediate medical attention.

Watch that video to know if it is safe to have sex during pregnancy or not
Alzheimer Disease Effects

-Rapidly progressive weakness of the lower extremities following an upper respiratory infection, accompanied by sensory loss and urinary retention, is characteristic for transverse myelitis.
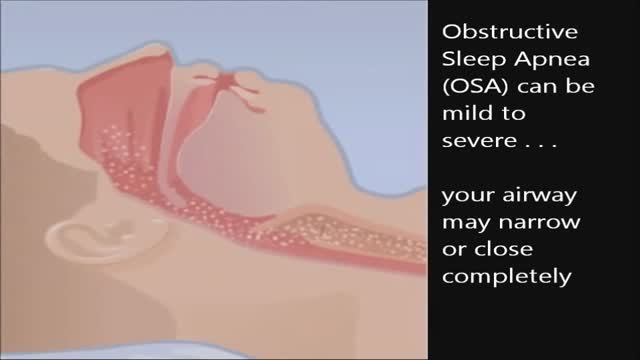
CPAP, or continuous positive airway pressure, is a treatment that uses mild air pressure to keep the airways open. CPAP typically is used by people who have breathing problems, such as sleep apnea. CPAP also may be used to treat preterm infants whose lungs have not fully developed.
Meningococcal meningitis - causes, features, symptoms and treatment
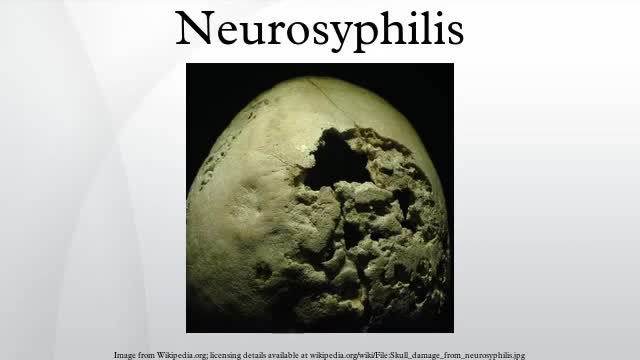
Neurosyphilis is an infection of the brain or spinal cord caused by the spirochete Treponema pallidum. It usually occurs in people who have had chronic, untreated syphilis, usually about 10 to 20 years after first infection and develops in about 25%–40% of persons who are not treated. The United States' Centers for Disease Control and Prevention (CDC) advises that neurosyphilis can occur at any stage of a syphilis infection.

Robot Flies Like a Bird
Eosinophilic granulomatosis with polyangiitis (EGPA; also known as Churg-Strauss syndrome [CSS] or allergic granulomatosis) is a rare autoimmune condition that causes inflammation of small and medium-sized blood vessels (vasculitis) in persons with a history of airway allergic hypersensitivity (atopy).
Type 2 Diabetes Animation 3D
