- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
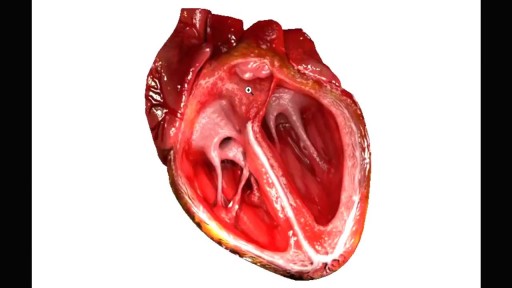
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Majority of patients these days prefer PCNL ( Minimal Invasive Telescopic removal of kidney stones broken with lithoclast, removed through a button hole incision ). This patient with a big stone in the pelvis of the kidney wanted it open only so I did an open pyelolithotomy for this patient after a long time as I use to do it in routine in the past. Except for the long incision and scar as compared to PCNL the recovery time was the same and patient went home third day happily walking and eating.

Butt implants are a popular plastic surgery procedure among those who wish to enhance the appearance, shape, and size of their rear ends. Buttock augmentation involves the surgical insertion of artificial body implants into a patient’s buttocks to create a larger, shapelier, and more sensuous rear end. Patients who have underdeveloped buttocks can achieve a more proportionate figure with butt implants. Women who wish to achieve an “hour glass” figure or are unhappy with the size of their buttocks can benefit from female butt implants. Men with flat or poorly developed buttocks can enhance the shape of the area to their liking with male butt implants. Many buttock augmentation patients say that their clothes fit better, they feel more attractive, and their confidence levels have improved.

Penile implants are devices placed inside the penis to allow men with erectile dysfunction (ED) to get an erection. Penile implants are typically recommended after other treatments for ED fail. There are two main types of penile implants, semirigid and inflatable.

Dysfunction in the sacroiliac joint, also called the SI joint, can sometimes cause lower back and/or leg pain. Leg pain from sacroiliac joint dysfunction can be particularly difficult to differentiate from radiating leg pain caused by a lumbar disc herniation (sciatica) as they can feel quite similar.

Curious about physiotherapy or wanting to know how to properly perform an exercise? Check us out on Social Media! Facebook: https://www.facebook.com/striveptandperformance/ Instagram: https://www.instagram.com/striveptandperf/ Twitter: https://twitter.com/StrivePTandPerf Blog: http://www.strivept.ca/blog

Bullae resection for right pneumothrax via VATS
Getting the right diagnosis often isn’t easy for psychiatric conditions. In our field, we don’t yet have biologic tests that can easily define one condition from another. If your blood pressure is 140 over 90, you have hypertension or high blood pressure. In mental health, we have to rely on a description of patterns or symptoms to makes diagnoses. This model is fraught with challenges. Without a clear biological model to work from, and given the complexity of the human brain, the field has settled upon dividing these descriptions of symptoms into syndromes. The Diagnostic and Statistical Manual of Mental
EKG/ECG Interpretation Explained Clearly

To avoid pregnancy and STDs, always remember to use a condom every time you have sex — including oral, vaginal, or anal sex. Whenever oral sex is being performed on a girl, a dental dam should be used. A guy receiving oral sex should wear a latex condom — or, if he or his partner is allergic to latex, a polyurethane condom.



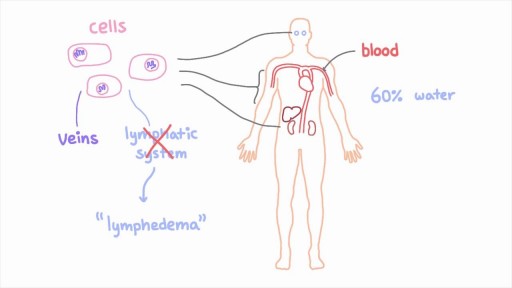
The lymphatic system is a network of specialized vessels (lymph vessels) throughout the body whose purpose is to collect excess lymph fluid with proteins, lipids, and waste products from the tissues. This fluid is then carried to the lymph nodes, which filter waste products and contain infection-fighting cells called lymphocytes. The excess fluid in the lymph vessels is eventually returned to the bloodstream. When the lymph vessels are blocked or unable to carry lymph fluid away from the tissues, localized swelling (lymphedema) is the result.
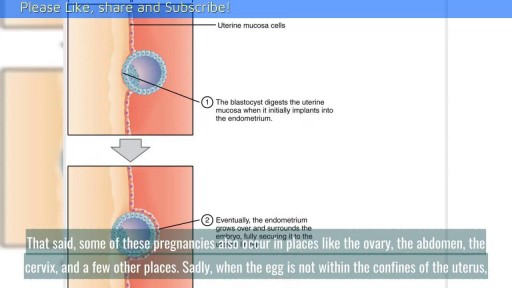
When Does Implantation Occur in Pregnancy? || Common gynaecological problems in women There are a lot of things going on in early pregnancy. The first thing that you need to understand is the menstrual cycle. A good understanding of this can help you understand how the other parts play into the process. A huge part of the menstrual cycle that is the basis of pregnancy is ovulation. Ovulation typically occurs fourteen days prior to the beginning of menstruation, the point when the uterine lining is sloughed off if no pregnancy has occurred.

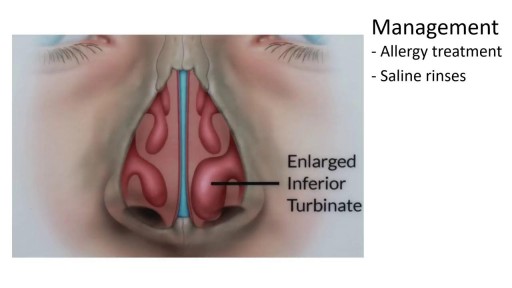
This video demonstrates how a broken nose is fixed using only local anesthesia and without sedation. Of course, this can also be performed while asleep.

Infected Tattoo Abscess


Synthol, otherwise known as site enhancement oil is used by some people (including bodybuilders) to increase the apparent size of their muscles by directly injecting the oil into their muscle tissue. Users treat it as a short cut of looking like a body builder, without the actual hard work of bodybuilding training. With repeated injections, a larger volume of synthol builds up inside the muscle, expanding its size like a balloon filling up with air. Side effects of synthol can cause nerve damage, stroke, ulcers, pulmonary embolisms, and much more. Injecting synthol is very dangerous and if that doesn’t deter potential users, there is also a problem from an aesthetic standpoint; synthol use makes ones body look deformed (just see for yourself in the pictures below).

How to Use Tampons for The First Time Demo Video
