- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Vaginal Speculum and Bimanual Exam

Gallstone ileus is an important, though infrequent, cause of mechanical bowel obstruction, affecting older adult patients who often have other significant medical conditions. It is caused by impaction of a gallstone in the ileum after being passed through a biliary-enteric fistula. The diagnosis is often delayed since symptoms may be intermittent and investigations fail to identify the cause of the obstruction. The mainstay of treatment is removal of the obstructing stone after resuscitating the patient. Gallstone ileus continues to be associated with relatively high rates of morbidity and mortality.
Lack of sunshine causes skin cancer, according to Andreas Moritz. In this video from 2009, he explains why being in the sun is actually good for you and your skin. Find out why your sunscreen is doing more harm than good. Also, you need vitamin D to prevent cancer, and sunscreen may interfere with your exposure to vitamin D from the sun.

Plantar warts are hard, grainy growths that usually appear on the heels or balls of your feet, areas that feel the most pressure. This pressure also may cause plantar warts to grow inward beneath a hard, thick layer of skin (callus). Plantar warts are caused by the human papillomavirus (HPV). The virus enters your body through tiny cuts, breaks or other weak spots on the bottom of your feet. Most plantar warts aren't a serious health concern and may not require treatment. But plantar warts can cause discomfort or pain. If self-care treatments for plantar warts don't work, you may want to see your doctor to have them removed.

TransMedics’ proprietary Organ Care System (OCS) is the first commercial and portable warm blood perfusion organ transport system. With the OCS, doctors are able to perform “living organ transplants,” where organs are kept warm and functioning in a controlled environment from the time they are recovered to the moment they are placed in the recipient’s body.
Genipap. A home pap smear product demo.

How Hair can be retsored and transplanted? natural versus biofibers?
Dr. Mohamed El Ruby
Consultant of Plastic Surgery - Ain Shams University

Asthma Mechanism 3D
Watch that video to know What is Vaginal Discharge and How To Get Rid Of It?
How we went from super species to the sickest. What gravity has to do with it.

EART (Health Education and Rescue Training) Wilderness First Aid is an intensive course that covers patient examination and evaluation, body systems and anatomy, wound care, splinting, environmental emergencies, and backcountry medicine. Hands-on simulations provide first-hand training in treating patients. This is an excellent course taught by experienced Wilderness First Responders and Emergency Medical Technicians and is highly recommended to all wilderness travelers. People who pass the courses will receive a Wilderness First Aid certification from the Emergency Care and Safety Institute (ECSI) which is good for 2 years. Participants who successfully pass CPR and HEART Wilderness First Aid will have met the First Aid requirements for OA Leader Training.

Watch that video to know the Natural Ways to Whiten Teeth at Home

http://www.landging.com/breast-augmentation-animation.html4
This breast augmentation animation demonstrates the procedure of saline breast implants.
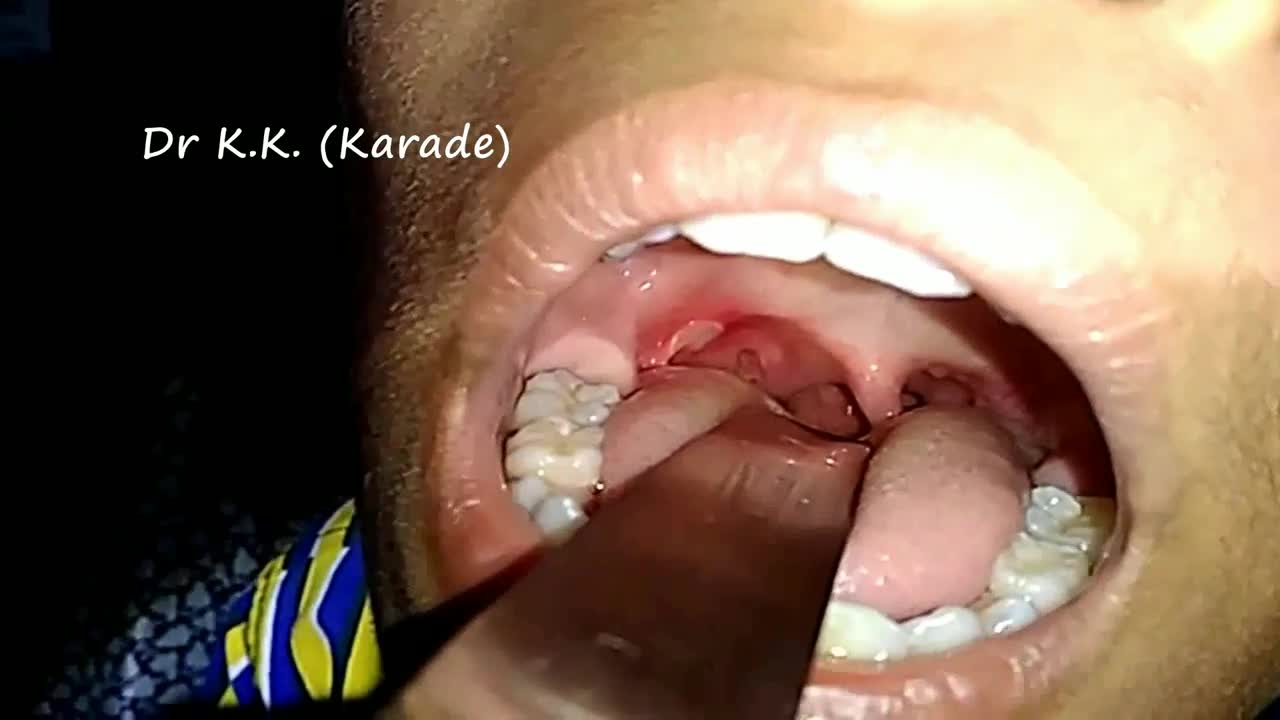
Canker sores (Aphthous ulcer) are small, painful ulcers on the inside of the mouth, tongue, lips, or throat.Canker sores are white or yellow and surrounded by a bright red area. They are not cancerous.
مرکز ایمپلنت و زیبایی دندان شیراز دکتر محمد امین دین پرور
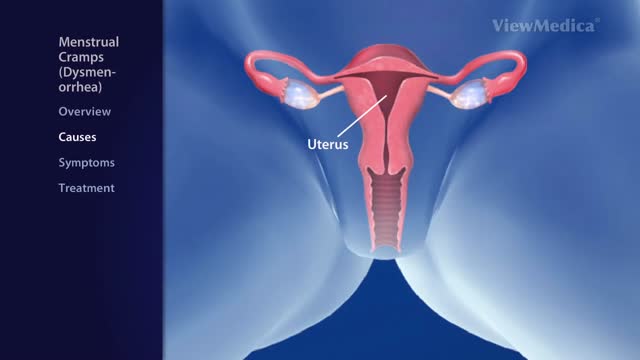
Dysmenorrhea is the medical term for pain with menstruation. There are two types of dysmenorrhea: "primary" and "secondary". Primary dysmenorrhea is common menstrual cramps that are recurrent (come back) and are not due to other diseases. Pain usually begins 1 or 2 days before, or when menstrual bleeding starts, and is felt in the lower abdomen, back, or thighs. Pain can range from mild to severe, can typically last 12 to 72 hours, and can be accompanied by nausea, vomiting, fatigue, and even diarrhea. Common menstrual cramps usually become less painful as a woman ages and may stop entirely if the woman has a baby. Secondary dysmenorrhea is pain that is caused by a disorder in the woman's reproductive organs, such as endometriosis, adenomyosis, uterine fibroids, or infection. Pain from secondary dysmenorrhea usually begins earlier in the menstrual cycle and lasts longer than common menstrual cramps. The pain is not typically accompanied by nausea, vomiting, fatigue, or diarrhea.
Emphysema gradually damages the air sacs (alveoli) in your lungs, making you progressively more short of breath. Emphysema is one of several diseases known collectively as chronic obstructive pulmonary disease Smoking is the leading cause of emphysema. Your lungs' alveoli are clustered like bunches of grapes. In emphysema, the inner walls of the air sacs weaken and eventually rupture — creating one larger air space instead of many small ones. This reduces the surface area of the lungs and, in turn, the amount of oxygen that reaches your bloodstream. When you exhale, the damaged alveoli don't work properly and old air becomes trapped, leaving no room for fresh, oxygen-rich air to enter. Treatment may slow the progression of emphysema, but it can't reverse the damage.

At first, grasping the needle is difficult because it will have a tendency to want to jump around. What can oftentimes help is to get hold of the thread with the left-hand forceps at a point 2 to 3 cm away from the needle. Dangle the needle until it just comes to rest on the surface. This will then allow you to use the angulated needle holder to grab the needle easily. Your needle is in a stable position if it is set up to 90 degrees to the axis of the tips of the forceps. You can make minor corrections by touching the needle with your left-hand forceps, or by partially relaxing your grip and nudging the needle tip against another firm object. You should hold the needle just behind its midpoint (If you hold it too near the tip, it will point downward. If you hold it too near the thread end, it will point upward.).
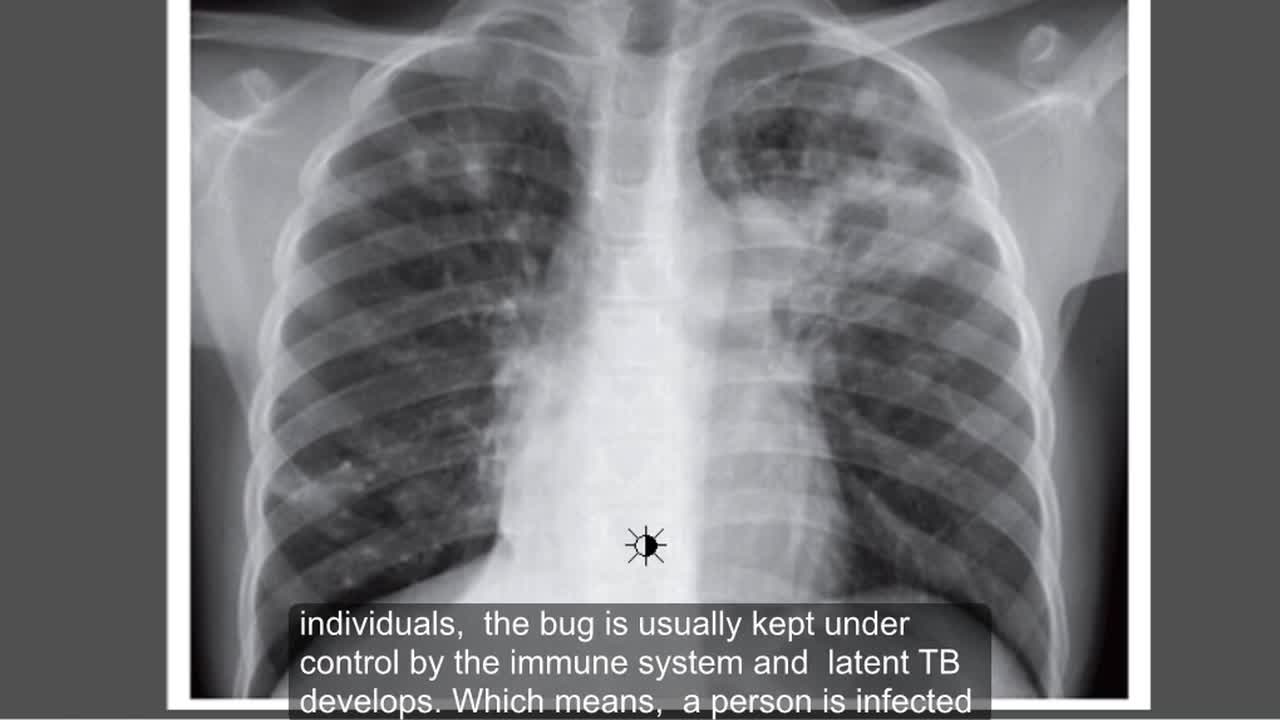
Tuberculosis (TB) is a potentially serious infectious disease that mainly affects your lungs. The bacteria that cause tuberculosis are spread from one person to another through tiny droplets released into the air via coughs and sneezes.
Minor burns can typically be treated at home -- but it's important to know when you need to seek treatment.
