- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Recent researches shows that women with periodontal disease are more prone to deliver premature babies

Recovery position
Anatomy of Love

Cerebellar functions of the upper limbs from the USMLE collection

A heart transplant, or a cardiac transplant, is a surgical transplant procedure performed on patients with end-stage heart failure or severe coronary artery disease when other medical or surgical treatments have failed.
http://smoking-videos.plus101.com
Quit Smoking Forever Formula Videos - How To Quit Smoking In As Fast As 1 Week Without Agitation, Cravings Or Withdrawal Symptoms.You're about to uncover the 3 elements that will rapidly boost your chances of success to quit smoking and not only that, you'll learn ways to escape cravings and how to avoid a relapse that can happen in the future even to people with the most willpower.
Arthritis of the hip causes severe pain, and sometimes requires surgical treatment, including hip replacement. This animated video show you what hip arthritis is, and how it causes symptoms.

FemTouch Vaginal Rejuvenation Laser
General Neurological Exam Power Reflex Sensory Cranial erves

Sex easily falls to the wayside during pregnancy. Research shows that good sex has a significant impact upon not just the relationship, but also a woman’s ability to have an easeful and even joyful birth. Unfortunately, sex during pregnancy can be quite complicated for a variety of physical and emotional reasons. This week’s video will outline how to overcome these hurdles and make sure you continue to enjoy the wonders of sex as you embark on the first steps of parenthood.
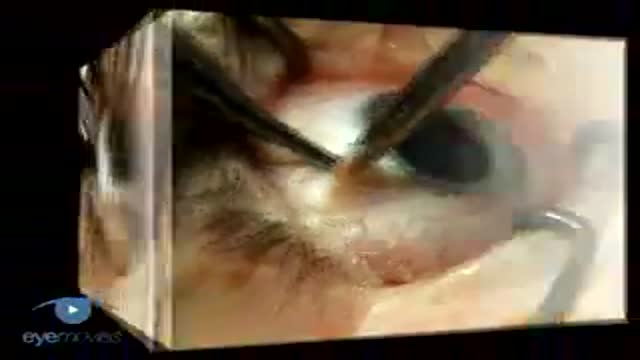
Scleral Buckling: Slinging Muscles & Marking Breaks VR1 Basic Techniques

Percutaneous Endoscopic Colostomy
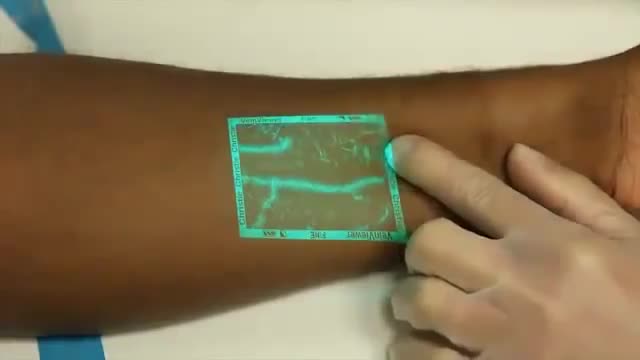
Venipuncture can be a challenging process for medical professionals especially when a patients veins are difficult to see. VeinViewer uses near infrared light to create a digital image of patient vasculature in real time.
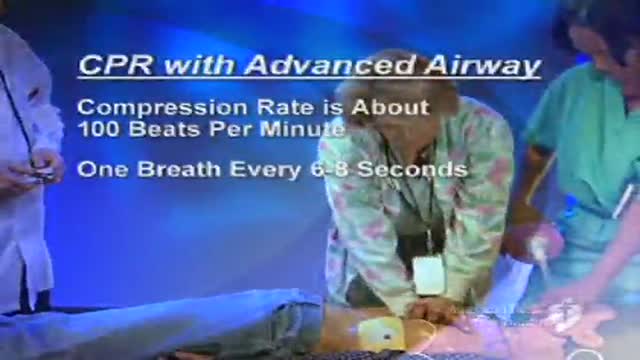
CPR in a patient with Advanced Airway Managment such as a patient with endotracheal tube or combitube is different than performin normal CPR. This video shows how to perform that.

Examination of Cranial nerve VIII: vestibulocochlear
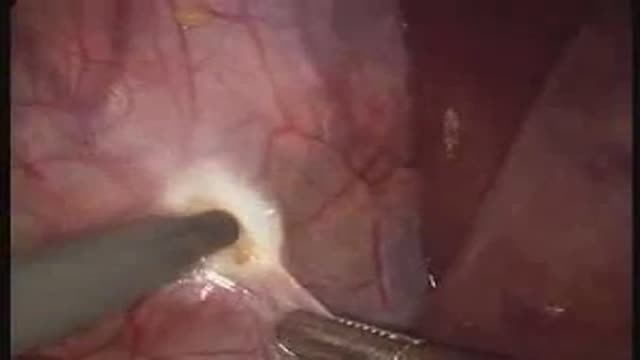
removal of a "toxic" phaeochromocytoma

DMC Pediatric Orthopaedic Surgery specialist repairs a youg girl's traumatic spine injury. ~ Detroit Medical Center

Less pain and no incisions are just two benefits of robotically assisted surgery thanks to the da Vinci Surgical System. ~ Detroit Medical Center

Lung Vasculature

