- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
These are a few common types of benign bone tumors: Osteochondroma is the most common benign bone tumor. ... Giant cell tumor is a benign tumor, typically affecting the leg (malignant types of this tumor are uncommon). Osteoid osteoma is a bone tumor, often occurring in long bones, that occurs commonly in the early 20s.

http://control-blood-sugar.good-info.co Normal Blood Sugar, Normal Blood Glucose, Low Blood Glucose, Foods That Lower Blood Sugar. happy to tell you that all these conditions of your uncontrollable blood sugar can be completely thrown away for good! Without expensive and dangerous surgery. Without leaving embarrassing pricking scars on your fingers. Without spending hundreds or even thousands of dollars on prescription drugs that not only empty your bank account. but leave big pharmaceutical executives richer from preying off your condition. The truth is, all of the blood sugar problems you’re having are completely reversible and curable. All of the frustrations and anxiety that comes with your condition can be a thing of the past. Plus, keep reading and you’ll find out the real truth to why prescription drugs are not helping your body control your blood sugar, but are guaranteed to ruin your body’s functions over time. you how to naturally and safely control your uncontrollable blood sugar in as little as 3 weeks. click here. http://control-blood-sugar.good-info.co

دكتور مصطفى ياقوت فى حوار على القناة الفضائية المصرية عن الطب البديل و الطب الفرعونى فى علاج الأرق
TV interview with Dr. Mostafa Yakoot about Alternative medicine

Ellie was born with a rare condition which stopped her jawbones from growing properly. At first, her parents didn't realize there was a problem, apart from the fact that her teeth were not aligned. But when she went to have braces fitted to straighten her teeth when she was 14, orthodontist Joy Hickman realized her jaw had not grown since she was eight. Over the next six years Hickman worked with a maxillofacial surgeon to transform Ellie's looks. Ellie, who is now 20, said the surgery was painful but paid almost immediate dividends. "About six months after it was my year 11 prom and it looked good." Ellie told the Daily Post the change in her appearance has been matched by an increase in confidence.

Watch that video of Butt and Legs Implants Exploded Inside Brazilian Model
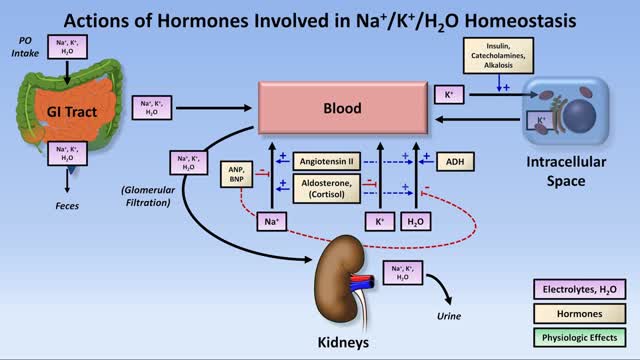
Low potassium (hypokalemia) refers to a lower than normal potassium level in your bloodstream. Potassium is a chemical (electrolyte) that is critical to the proper functioning of nerve and muscles cells, particularly heart muscle cells. Normally, your blood potassium level is 3.6 to 5.2 millimoles per liter (mmol/L). A very low potassium level (less than 2.5 mmol/L) can be life-threatening and requires urgent medical attention.
A young patient undergoes state of the art robotic surgery for Ovarian Cancer and Endometrial Cancer in Chicago, IL. The surgery is performed by noted gynecologic oncologist and expert robotic surgeon M. Patrick Lowe MD. Dr Lowe has been performing robotic surgery since 2006 and is one of a few gynecologic oncologist in the United States who utilizes robotics for ovarian cancer.

Demonstration of simple interrupted suturing technique for laceration repair.

laparoscopic left adrenalectomy in 150kg patient with Cushings

BIG wart blister after freezing with liquid nitrogen

Massive Tumor Removed from Man's Face

A Cesarean section (C-section) is surgery to deliver a baby. The baby is taken out through the mother's abdomen. In the United States, almost one in three women has their babies this way. Some C-sections are planned, but many are done when unexpected problems happen during delivery. Reasons for a C-section may include

Dr. Yeong Kwok speaks about knee pain and demonstrates a stretch designed to treat tendonitis.


Rhabdomyolysis is a condition in which damaged skeletal muscle (Ancient Greek: rhabdomyo-) tissue breaks down rapidly (Greek –lysis). This damage may be caused by physical (e.g. crush injury), chemical, or biological factors. Breakdown products of damaged muscle cells are released into the bloodstream; some of these, such as the protein myoglobin, are harmful to the kidney and may lead to kidney dysfunction. The severity of the symptoms (which may include muscle pains, vomiting and confusion) depends on the extent of the muscle damage, and whether kidney failure develops. The mainstay of treatment is generous intravenous fluids, but could include dialysis or hemofiltration.
Rhabdomyolysis and its complications are significant problems for those injured in disasters such as earthquakes and bombing. Relief efforts in areas struck by earthquakes often include medical teams with skills and equipment for treatment of survivors with rhabdomyolysis. The disease and its mechanisms were first fully elucidated during the Blitz of London in 1941.
Systemic Lupus Erythematosus (SLE)information

fixation of a tibial fracture utilizing the Titanium Cannulated Tibial Nail

Atherosclerosis is a narrowing of the arteries caused by a buildup of plaque. It’s also called arteriosclerosis or hardening of the arteries. Arteries are the blood vessels that carry oxygen and nutrients from your heart to the rest of your body. As you get older, fat and cholesterol can collect in your arteries and form plaque. The buildup of plaque makes it difficult for blood to flow through your arteries. This buildup may occur in any artery in your body and can result in a shortage of blood and oxygen in various tissues of your body. Pieces of plaque can also break off, causing a blood clot. Atherosclerosis can lead to heart attack, stroke, or heart failure if left untreated.

During 34 week of pregnancy, the baby is getting ready for delivery, you may feel less wriggling and kicking. Watch out this video to learn more about being 34 weeks pregnant.

Female Reproductive System Anatomy
