- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

St. Luke's originally broadcast this live in a webcast and later re-purposed it for air on KCRG-TV9 as an educational video. It is hosted by Ashley Hinson, KCRG-TV9 anchor and Dr. Sandeep Munjal. Dr. Jeff Nassif performs the knee replacement surgery on an eastern Iowa woman. St. Luke's has a rapid recovery joint replacement program, which gets people back to life quickly after surgery.

Women's College Hospital is revolutionizing the way knee-replacement surgery is done. It is starting to provide the procedure as an ambulatory service. Patients can go home from hospital four hours after having the surgery. In some other hospitals knee replacement surgery patients have to stay as long as 4 days.
Read an excerpt from Theresa Boyle's story:
It’s been less than four hours since Greg Nemez underwent knee-replacement surgery and the 56-year-old Mississauga man is already on his way home from hospital.
This past Monday, he became the fifth patient at Toronto’s Women’s College Hospital to undergo the outpatient procedure, which normally requires a hospital stay of two or three days.
“I’m happy ... You have that freedom of movement from before. It’s like wow,” he said on the elevator as he was leaving the hospital.
After years of being unable to hold his leg straight, the real-estate agent can finally do so. A 20-year-old football injury had left him with severe arthritis and pain.
Read the full story:
https://www.thestar.com/news/g....ta/2018/04/11/he-got
Follow the Toronto Star on social media:
Facebook: https://www.facebook.com/torontostar/
Twitter: https://twitter.com/TorontoStar
Instagram: https://www.instagram.com/thetorontostar/

A recap of Mater Hospital patient Helen's story as she progressed from experiencing chronic knee pain due to osteoarthritis, through to knee replacement treatment and ultimately a new lease on life.
Dedicated to surgical excellence and patient-centred care, the Mater Hospital North Sydney is regarded as a leading orthopaedic hospital and the only Australian hospital to be accepted into the International Society of Orthopaedic Centres.
For more information, click here: https://bit.ly/3bvhY8G


In this animated episode of eOrthopodTV, orthopedic surgeon Randale C. Sechrest, MD narrates the procedure to replace an arthritic knee with an artificial joint.

Mohs Surgeon Dr. Leslie Christenson shows entire Mohs Surgery from start to finish. This is the full procedure and includes the entire surgery. Dr. Christenson talks about the procedure as she removes the skin cancer.
Learn more about Dr. Christenson: https://www.mcfarlandclinic.co....m/doctors/leslie-chr
Learn more about Mohs Surgery: https://www.mcfarlandclinic.co....m/doctors/specialtie

Three to five years after gastric bypass surgery, some patients start to regain weight because the size of their stoma (the opening at the bottom of the stomach pouch) or their stomach pouch itself has increased. This can keep you from feeling full after small meals.
To resolve this problem, our surgeons use new surgical tools to create and suture folds into the pouch, reducing its volume and at the stoma to decrease its diameter. The surgeon performs the procedure entirely through the mouth -- inserting an endoscope under heavy sedation -- so there are no external incisions into the body.

For a full Surgical Airway Techniques resource: https://bit.ly/2rb9Nud
Video courtesy of Gauri Mankekar, MBBS, MS, PhD

Lattrell Wells was a perfect candidate for the MACI procedure. Dr. Michael O'Malley is a sports medicine surgeon at Carilion Clinic, "It’s a two stage procedure. So what we do is we actually harvest a small portion of the patient's cartilage and bone cells and we send it to a lab where the lab then that grows additional cartilage cells. It comes back to us in a little sheet and six weeks after that initial surgery, we re-implant the cartilage in a second surgery where we implant that sheet depending on the size of lesion right where his defect. This the only option where there’s virtually no risk of any kind of graft rejection or anything of that nature.

Lumpectomy means that a focal area of cancer is going to be removed. A lot of patients with a lumpectomy don’t need any specific breast reconstruction, explains Dr. Miguel Angel Medina, Director of Microsurgery with Miami Cancer Institute.
Al the end of surgical treatment, all those patients go on to need radiation therapy. For patients who have large breasts, physicians have to take a larger lumpectomy than normal.

How to perform a parotidectomy gland resection? In this video we take you step by step through the protid gland resection surgical technique. This video is intended for ENT residents and Head and Neck Surgery Surgeons. It is part of the ORL-Information's Head and Neck surgery Masterclass in collaboration with the University Hospital of Nîmes. Surgeons Editors: Pr. Benjamin LALLEMANT, MD, PhD - Dr. Camille GALY, MD Head and and Neck Department, University Hospital of Nîmes, France Official video | www.orl-information.fr
Cette vidéo présentent la technique de la parotidectomie avec dissection du nerf facial. Elle illustre les différents temps de l'intervention notamment le temps de repérage du nerf facial.
--------------------------------------
@Prévention médecine | Comment préserver sa santé ?
✔Abonnez-vous à la chaîne ORL-Information : https://www.youtube.com/c/ORLINFORMATION
✔Retrouvez-nous sur internet: https://www.orl-information.fr

Orthopedic spine surgeons and vascular surgeons at UW Health in Madison, WI work together to perform minimally invasive anterior lumbar interbody fusion (Mini-ALIF). With this type of spinal fusion surgery, patients have smaller incisions, usually spend less time in the hospital and typically return to daily activities more quickly. Learn more https://www.uwhealth.org/ALIF

It used to be when a woman needed a hysterectomy she could expect full abdominal surgery with a long recovery time. Dr. Melissa Lee uses less invasive methods that can cut the patients downtime in half.
"We were trained in more laparoscopic and minimally invasive cases so of course that's what I'm more comfortable with doing right now."
She sees a new generation of patients opting for laparoscopic surgery.
"Laparoscopy is the use of small cameras with small incisions and instruments that are guided by the hand, and you're able to see directly into the abdomen without actually fully opening the abdomen," says Dr. Lee, an obstetrician-gynecologist with Lee Memorial Health System.
Nowadays, even a large mass or uterus can be removed using the slender tools.
"There are multiple different laparoscopic instruments that you can use. Whether they're blunt dissections or just dissectors that hold and retract back or actual scissors or cutting instruments, there are multiple different options," says Dr. Lee.
While a standard abdominal hysterectomy requires a four to eight inch incision, the laparoscope needs only a quarter to half inch. It's enough to make a big difference in terms of recovery.
"They're able to get up and move around faster. They're able to recover faster, their pain level and their need for pain medicine is much lower," says Dr. Lee.
The laparoscopic procedure also cuts down on scarring and more importantly, shortens the hospital stay. The trend now is home within 24 hours.
"Where the patient is done early in the morning, they're doing well they're tolerating oral intake they're able to getup and move around. And those patients a lot of times will feel comfortable to go home that same nigh after a major surgery," says Dr. Lee.
New studies show women who've had a laparoscopic hysterectomy viewed their quality of life as better than those who had an open abdominal procedure, making this a good option for the right patient.
View More Health Matters video segments at leememorial.org/healthmatters/
Lee Memorial Health System in Fort Myers, FL is the largest network of medical care facilities in Southwest Florida and is highly respected for its expertise, innovation and quality of care. For nearly a century, we've been providing our community with everything from primary care treatment to highly specialized care services and robotic assisted surgeries.
Visit leememorial.org
They are the leaders of the pack when it comes to minimally invasive surgeries. Laparoscopic and robotic. Different techniques with the same benefits.
"There's significantly less blood loss, it's a quicker procedure, quicker recovery, less scarring, less chance for post operative wound complications or infections," says Dr. Darren Miter, laparoscopic surgeon with Lee Memorial Health System.
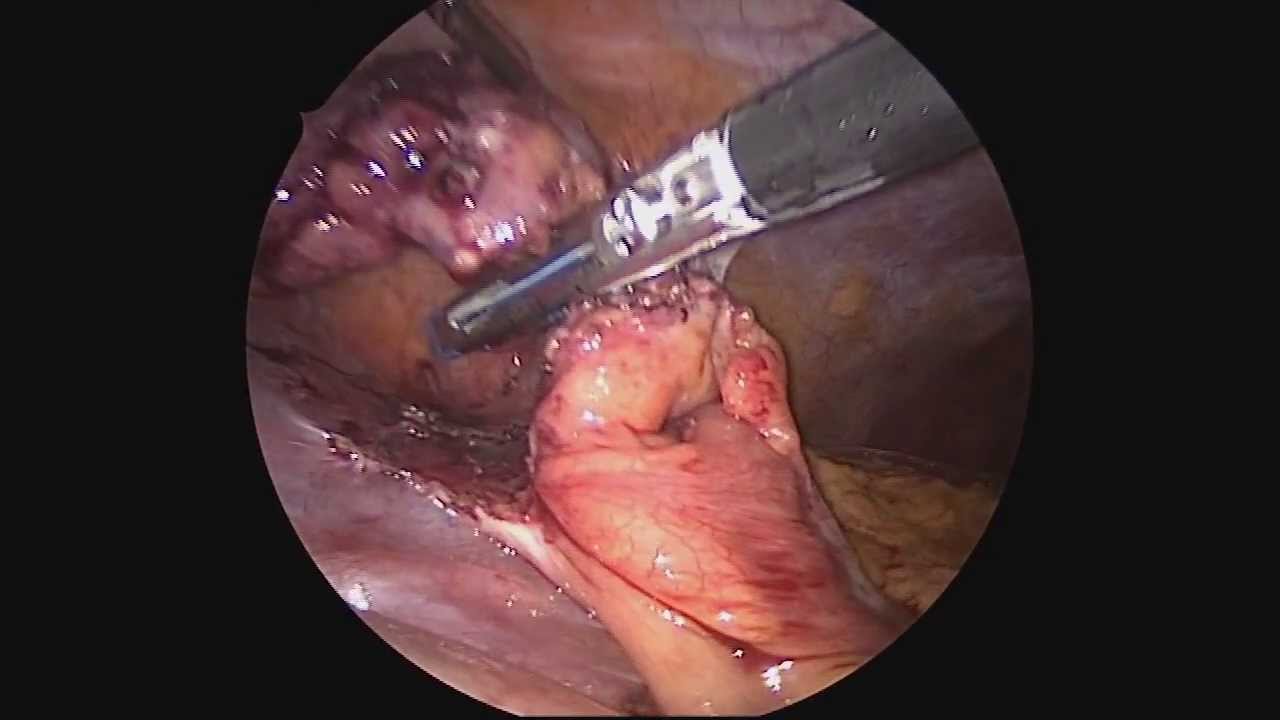
In a laparoscopic procedure surgeons operate through a series of poke holes, manually inserting thin cutting tools and a camera to provide magnified vision. It's used in a variety of surgical specialties.
"The vast majority of gallbladder surgeries are performed laparoscopically. A single incision in the belly button, one up under the breastbone and either one or two in the right upper side of the belly. Using long skinny instruments and looking up at a TV monitor, remove the gallbladder that way," says Dr. Miter.
While laparoscopic is a hands-on approach, robotic procedures are surgeon-controlled. Working at a console, surgeons direct the robotic arms, which have super-human capabilities and 3D, hi def vision.
"I mean you have to see it to believe it, that's a great tool to have. You got a very good depth perception. Plus the other thing when you're working with your hands it's more intuitive," says Dr. Nagesh Ravipati, colorectal surgeon with Lee Memorial Health System.
The robotic system performs maneuvers the human hand can't.
"Especially if you have to do any suturing, it is so much simpler with the robots because you can just turn around 360 degrees," says Dr. Ravipati.
Robotic surgery is gaining momentum in precise procedures, including the field of cancer.
"The robot is good when you're going to operate on just one field. For rectal surgery you're in one place, it's docked. It gives you the best 3 dimensional vision," says Dr. Ravipati.
Robotic and laparoscopic. Both cutting edge options, with less cutting.
View More Health Matters video segments at leememorial.org/healthmatters/
Lee Memorial Health System in Fort Myers, FL is the largest network of medical care facilities in Southwest Florida and is highly respected for its expertise, innovation and quality of care. For nearly a century, we've been providing our community with everything from primary care treatment to highly specialized care services and robotic assisted surgeries.
Visit leememorial.org
Dr. Celia Divino, Chief, Division of General Surgery at The Mount Sinai Hospital, performs a laparoscopic appendectomy. Visit the Division of General Surgery at http://bit.ly/18z944M. Click here to learn more about Dr. Celia Divino http://bit.ly/12RF0ee

Mini-Laparoscopic Cholecystectomy with Intraoperative Cholangiogram for Symptomatic Cholelithiasis (Gallstones) - Standard
Authors: Brunt LM1, Singh R1, Yee A2
Published: September 26, 2017
AUTHOR INFORMATION
1 Department of Surgery, Washington University, St. Louis, Missouri
2 Division of Plastic and Reconstructive Surgery, Washington University, St. Louis, Missouri
DISCLOSURE
No authors have a financial interest in any of the products, devices, or drugs mentioned in this production or publication.
ABSTRACT
Minimal invasive laparoscopic cholecystectomy is the typical surgical treatment for cholelithiasis (gallstones), where patients present with a history of upper abdominal pain and episodes of biliary colic. The classic technique for minimal invasive laparoscopic cholecystectomy involves four ports: one umbilicus port, two subcostal ports, and a single epigastric port. The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) has instituted a six-step strategy to foster a universal culture of safety for cholecystectomy and minimize risk of bile duct injury. The technical steps are documented within the context of the surgical video for (1) achieving a critical view of safety for identification of the cystic duct and artery, (2) intraoperative time-out prior to management of the ductal structures, (3) recognizing the zone of significant risk of injury, and (4) routine intraoperative cholangiography for imaging of the biliary tree. In this case, the patient presented with symptomatic biliary colic due to a gallstone seen on the ultrasound in the gallbladder. The patient was managed a mini-laparoscopic cholecystectomy using 3mm ports for the epigastric and subcostal port sites with intraoperative fluoroscopic cholangiogram. Specifically, the senior author encountered a tight cystic duct preventing the insertion of the cholangiocatheter and the surgical video describes how the author managed the cystic duct for achieving a cholangiogram, in addition to the entire technical details of laparoscopic cholecystectomy.

This surgical animation is for patient education and describes a laparoscopic colectomy, which is a type of minimally invasive surgery for colon cancer. Laparoscopic colectomy, also called minimally invasive colectomy, involves several small incisions in your abdomen. Instead of a big incision, the surgeon makes a few small cuts (0.5-1 centimeters) in the abdominal cavity to insert a surgical camera and instruments and perform the operation. A slightly bigger incision, about 3.5 centimeters wide, is made to remove the tumor.
When compared to traditional open surgery, laparoscopic colectomy can result in much less pain and swifter recovery. Depending on the procedure, most laparoscopic colectomy patients leave the hospital and return to normal activities more quickly than patients recovering from open surgery.
Colorectal cancer is the second leading cause of cancer death in the United States.
For more information about 3d animation videos, please visit https://www.amerra.com

"Laparoscopic Placement of a
Peritoneal Dialysis Catheter"
Houston Methodist DeBakey Heart & Vascular Center, presents a cardiovascular procedure featuring Eric K. Peden, MD, Shri Timbalia, MD, and Kenneth Livingston as they demonstrate “Laparoscopic Placement of a
Peritoneal Dialysis Catheter".
Surgery: Eric K. Peden, MD, Shri Timbalia, MD, and Kenneth Livingston
Narration: Kenneth Livingston
** This medical education program may contain graphic content. **
_________________________________
A DeBakey CV Education event
Presented by Houston Methodist DeBakey Heart & Vascular Center.
Building on Dr. Michael E. DeBakey’s commitment to excellence in education, Houston Methodist DeBakey CV Education is an epicenter for cardiovascular academic and clinical educational programs that support the provision of optimal care to patients suffering from cardiovascular conditions and diseases.
FOR MORE INFORMATION
DeBakey CV Education:
https://www.houstonmethodist.o....rg/education/medical
For the latest education and training opportunities from DeBakey CV Education: http://bit.ly/HMdebakeyemail
Follow Us:
Facebook: https://www.facebook.com/debakeycvedu
Twitter: https://twitter.com/DeBakeyCVedu
Livestream: https://livestream.com/debakey
SmugMug: https://debakey.smugmug.com/
Want concise, relevant reviews of the hottest topics in CV medicine? Subscribe for FREE to the Methodist DeBakey Cardiovascular Journal for quarterly, peer-reviewed issues delivered to your door.
https://journal.houstonmethodist.org/

This video demonstrates Laparoscopic Cholecystectomy Fully Explained Skin-to-Skin Video with Near Infrared Cholangiography performed by Dr R K Mishra at World Laparoscopy Hospital. A laparoscopic cholecystectomy is a minimally invasive surgical procedure that involves removing the gallbladder. It is typically performed using small incisions in the abdomen, through which a laparoscope (a thin tube with a camera and light) and surgical instruments are inserted. The surgeon uses the laparoscope to visualize the inside of the abdomen and to guide the instruments in removing the gallbladder.
Near-infrared cholangiography is a technique that uses a special camera and fluorescent dye to visualize the bile ducts during surgery. The dye is injected into the cystic duct (the tube that connects the gallbladder to the bile ducts) and the camera detects the fluorescence emitted by the dye, allowing the surgeon to see the bile ducts more clearly.
The combination of laparoscopic cholecystectomy and near-infrared cholangiography has become a standard of care in many hospitals and surgical centers. It allows for a more precise and efficient surgery, reducing the risk of complications such as bile duct injury.
The use of indocyanine green (ICG) with near-infrared imaging during laparoscopic cholecystectomy has several advantages. Here are some of them:
Better visualization of the biliary anatomy: ICG with near-infrared imaging allows for better visualization of the biliary anatomy during surgery. This helps the surgeon identify important structures, such as the cystic duct and the common bile duct, and avoid injuring them.
Reduced risk of bile duct injury: With better visualization of the biliary anatomy, the risk of bile duct injury during surgery is reduced. Bile duct injury is a serious complication that can occur during laparoscopic cholecystectomy and can lead to long-term health problems.
Improved surgical precision: ICG with near-infrared imaging also improves surgical precision. The surgeon can better see the tissues and structures being operated on, which can help reduce the risk of bleeding and other complications.
Shorter operating time: The use of ICG with near-infrared imaging can shorten the operating time for laparoscopic cholecystectomy. This is because the surgeon can more quickly and accurately identify the biliary anatomy, which can help streamline the surgery.
Overall, the use of ICG with near-infrared imaging is a valuable tool in laparoscopic cholecystectomy that can improve surgical outcomes and reduce the risk of complications.
Like any surgical procedure, laparoscopic cholecystectomy (gallbladder removal) has potential complications. Here are some of the most common ones:
Bleeding: Bleeding during or after the surgery is a possible complication of laparoscopic cholecystectomy. Most cases are minor and can be easily controlled, but in rare cases, significant bleeding may require a blood transfusion or even additional surgery.
Infection: Any surgical procedure carries a risk of infection. After laparoscopic cholecystectomy, there is a risk of infection at the site of the incisions or within the abdomen. Symptoms may include fever, pain, redness, or drainage from the incision sites.
Bile leakage: In some cases, a small amount of bile may leak from the bile ducts into the abdominal cavity after gallbladder removal. This can cause abdominal pain, fever, and sometimes requires further surgery or treatment.
Injury to nearby organs: During the surgery, there is a small risk of unintentional injury to nearby organs such as the liver, intestines, or bile ducts. This can cause additional complications and may require further treatment.
Adverse reactions to anesthesia: As with any surgery requiring general anesthesia, there is a small risk of adverse reactions to the anesthesia, such as an allergic reaction, respiratory problems, or heart complications.
Most patients recover without complications following a laparoscopic cholecystectomy, but it is important to discuss any concerns or questions with your surgeon beforehand.
Contact us
World Laparoscopy Hospital
Cyber City, Gurugram, NCR Delhi
INDIA : +919811416838
World Laparoscopy Training Institute
Bld.No: 27, DHCC, Dubai
UAE : +971525857874
World Laparoscopy Training Institute
8320 Inv Dr, Tallahassee, Florida
USA : +1 321 250 7653
Regenerate response

Dr. Lohith U, Consultant Surgical Gastroenterology, Bariatric and GI Oncology, Manipal Hospital Sarjapur, speaks about advanced laparoscopic surgery in this informative video. He shares details about the procedure,insights on its advantages, and how it can help treat gastrointestinal issues without making large incisions in a patient’s body. To know more watch this video.
Consult the experts here - https://bit.ly/3RiWqPr
#ManipalHospitalSarjapur #YourManipal #LifesOn #Healthcare #LaparoscopicSurgery
