- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Watch that video to know How to Treat Pimples on Your Face?

Watch that video of Doctors Removed 30 Pounds Of Poop From Man’s Colon

Watch that World's first osteotomy surgery for spine deformity

Verrugas En El Cuello, Como Borrar Lunares De La Cara, Como Quitar Las Verrugas Del Cuello --- http://sinverrugasylunares.plus101.com --- El Ajo Para Eliminar Las Verrugas, PRUEBALO!!! Antes que nada déjame comentarte que el ajo es un poderoso antiséptico, con propiedades fungicidas, bactericidas y también ayudan a depurar nuestro cuerpo. El ajo es rico en un compuesto llamado alicina, este elemento es un poderoso antivirus y anti bacterial natural, eso sin mencionar las propiedades antioxidantes que el ajo posee las cuales son de enorme beneficio para la salud de nuestra piel y por supuesto la salud en general. Es un tratamiento sencillo pero bastante efectivo, te recomiendo que lo comiences a partir de hoy mismo. Por las mañanas en ayunas tomate un ajo crudo, esto con el fin de limpiar nuestro organismo de virus y bacterias. Recuerda que nuestra misión es eliminar la raíz de las verrugas y los lunares tal como lo hablamos anteriormente el responsable de las verrugas es el virus del papiloma humano. El ajo gracias a sus propiedades antivirales nos ayudarán a combatir el virus desde adentro. Haz esto todos los días. Tomándote un ajo diario en ayunas estarás atacando el virus desde adentro, Ahora lo atacaremos desde fuera Para esto necesitarás un ajo, debes partirlo en porciones pequeñas calcula el tamaño de las porciones para cubrir los lunares y/o tus verrugas. Y ahora da a conocer el mismo método que él utilizó para curarse y eliminar las verrugas y lunares para siempre. Te invito a conocerlo a través del siguiente enlace: http://sinverrugasylunares.plus101.com

How to insert Endotracheal tube in children

Medication Through Running IV
Immunohistochemistry or IHC refers to the process of detecting antigens (e.g., proteins) in cells of a tissue section by exploiting the principle of antibodies binding specifically to antigens in biological tissues.[1] IHC takes its name from the roots "immuno," in reference to antibodies used in the procedure, and "histo," meaning tissue (compare to immunocytochemistry). Immunohistochemical staining is widely used in the diagnosis of abnormal cells such as those found in cancerous tumors. Specific molecular markers are characteristic of particular cellular events such as proliferation or cell death (apoptosis). IHC is also widely used in basic research to understand the distribution and localization of biomarkers and differentially expressed proteins in different parts of a biological tissue. Visualising an antibody-antigen interaction can be accomplished in a number of ways. In the most common instance, an antibody is conjugated to an enzyme, such as peroxidase, that can catalyse a colour-producing reaction. Alternatively, the antibody can also be tagged to a fluorophore, such as fluorescein or rhodamine

You can see more videos on ENT channel.

Robotic Prostatectomy Cornell Athermal Robotic Technique

Anatomy of The Leg and Foot
Anatomy of The Orbit
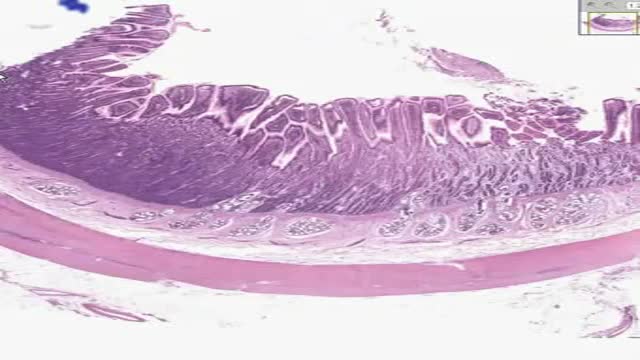
Histology of Small Intestine Duodenum

Top 10 Foods that Can Kill You
Head transplant successfully performed on monkey,
You may have a lot of questions about epilepsy. We will help you understand the basics, answer the most common questions, and help you find resources and other information you may need. However, information alone won’t help you manage your epilepsy and find a way to cope with the effects on your daily life. You’ll need to learn how to use the information and make it work for you.

The Babies Hooked On Heroin |
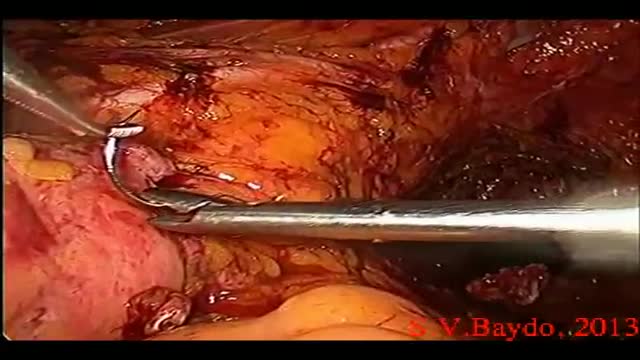
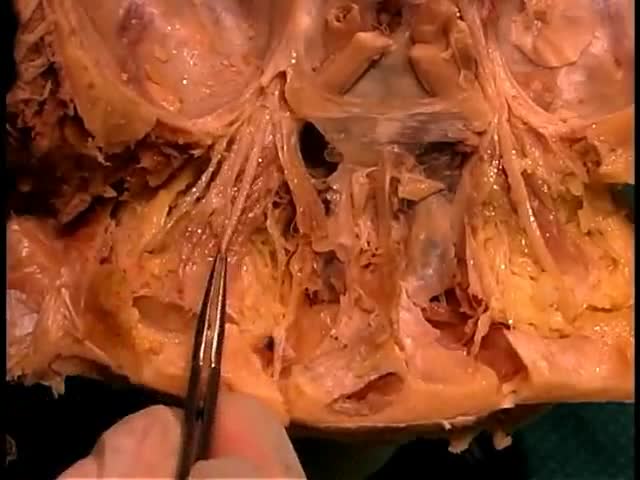
Iatrogenic injury to the ureter is a potentially devastating complication of modern surgery. The ureters are most often injured in gynecologic, colorectal, and vascular pelvic surgery. There is also potential for considerable ureteral injury during endoscopic procedures for ureteric pathology such as tumor or lithiasis. While maneuvers such as perioperative stenting have been touted as a means to avoid ureteral injury, these techniques have not been adopted universally, and the available literature does not make a case for their routine use. Distal ureteral injuries are best managed with ureteroneocystostomy with or without a vesico-psoas hitch. Mid-ureteral and proximal ureteral injuries can potentially be managed with ureteroureterostomy. If the distal segment is unsuitable for anastomosis then a number of techniques are available for repair including a Boari tubularized bladder flap, transureteroureterostomy, or renal autotransplantation. In rare cases renal autotransplantation or ureteral substitution with gastrointestinal segments may be warranted to re-establish urinary tract continuity. Laparoscopic and minimally invasive techniques have been employed to remedy iatrogenic ureteral injuries.
How To Cleanse Colon
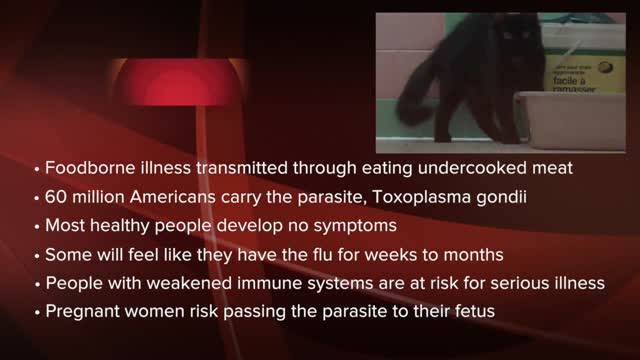
Toxoplasmosis (tok-so-plaz-MOE-sis) is a disease that results from infection with the Toxoplasma gondii parasite, one of the world's most common parasites. Toxoplasmosis may cause flu-like symptoms in some people, but most people affected never develop signs and symptoms. For infants born to infected mothers and for people with weakened immune systems, toxoplasmosis can cause extremely serious complications. If you're generally healthy, you probably won't need any treatment for toxoplasmosis. If you are pregnant or have lowered immunity, certain medications can help reduce the infection's severity. The best approach, though, is prevention.

Allergic bronchopulmonary aspergillosis (ABPA) is a condition characterised by an exaggerated response of the immune system (a hypersensitivity response) to the fungus Aspergillus (most commonly Aspergillus fumigatus). It occurs most often in patients with asthma or cystic fibrosis.
