- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
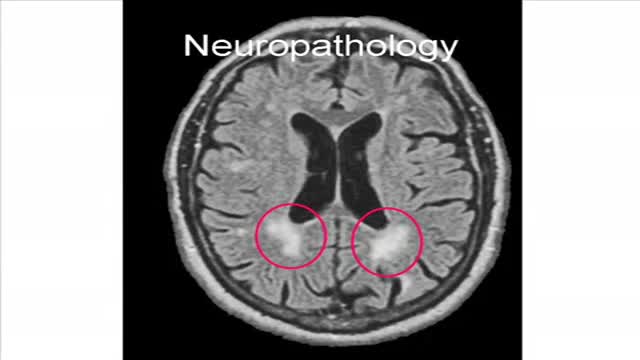
Binswanger's disease is a type of vascular dementia that involves white matter infarcts. Patients with this disease usually present with apathy, agitation, and bilateral corticospinal or bulbar signs
Panic attacks are discrete periods of intense fear or discomfort. Symptoms may include palpitations, sweating, trembling, shortness of breath, a choking sensation, chest pain, nausea, dizziness, paresthesias, and a fear of dying or losing control

If you suspect that you have sleep apnea, the usual first step is to discuss your suspicions with your primary care physician. If you don’t have a primary care physician, you can go directly to a clinician who is a sleep specialist. But check your health care insurance coverage first. Some policies require you to see a primary care physician first, and some policies limit the sleep centers and testing facilities whose services they will pay for. Unfortunately, you may discover that your policy offers limited or no coverage for the diagnosis and treatment of sleep apnea, in which case you may wish to switch insurers if and when you can.
Progressive multifocalleukoencephalopathy is a demyelinating illness of the central nervous system that typically occurs in immunosuppressed patients, especially those with AIDS. It is caused by reactivation of the polyomavirus JC (JC virus) and presents with neurologic deficits including hemiparesis, gait ataxia, visual symptoms, and altered mental status. It is not seen in non-immunosuppressed patients, and fever is not typical
Meningococcal meningitis - causes, features, symptoms and treatment
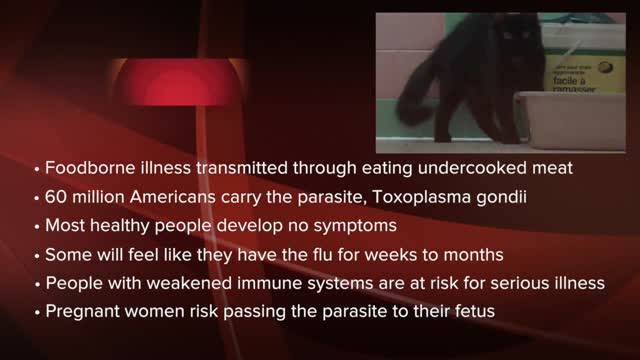
Toxoplasmosis (tok-so-plaz-MOE-sis) is a disease that results from infection with the Toxoplasma gondii parasite, one of the world's most common parasites. Toxoplasmosis may cause flu-like symptoms in some people, but most people affected never develop signs and symptoms. For infants born to infected mothers and for people with weakened immune systems, toxoplasmosis can cause extremely serious complications. If you're generally healthy, you probably won't need any treatment for toxoplasmosis. If you are pregnant or have lowered immunity, certain medications can help reduce the infection's severity. The best approach, though, is prevention.

ADC was first identified early in the AIDS epidemic as a common and novel CNS syndrome.(4,5) The three components of the term, AIDS dementia complex embody central features of the condition. AIDS emphasizes its morbidity and poor prognosis, particularly when its severity is at stage 2 or greater (see Table 1), a severity comparable to other clinical AIDS-defining complications of HIV-1 infection. Dementia designates the acquired and persistent cognitive decline with preserved alertness that usually dominates the clinical presentation and determines its principal disability. Complex emphasizes that this disease not only impairs the intellect, but also concomitantly alters motor performance and, at times, behavior. This involvement of the nervous system beyond cognition is evidence of a wider involvement of the CNS than occurs in some other types of dementia such as Alzheimer's disease. Additionally, myelopathy may be an important, indeed predominating, aspect of ADC, and organic psychosis may also be a feature in a subset of patients (see Rheumatologic and Musculoskeletal Manifestations of HIV). These manifestations are therefore also encompassed within this term. By contrast, neither neuropathy nor functional psychiatric disturbance are included in ADC.
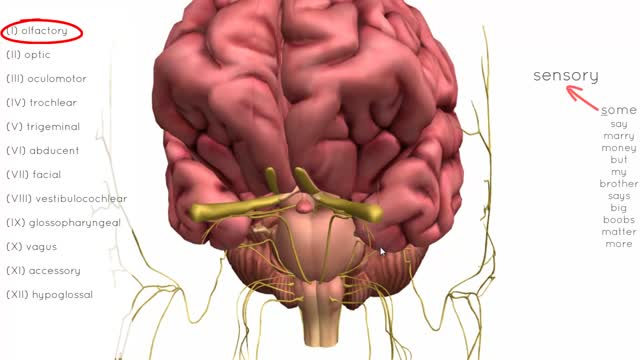
There are twelve cranial nerves in total. The olfactory nerve (CN I) and optic nerve (CN II) originate from the cerebrum. Cranial nerves III – XII arise from the brain stem (Figure 1). They can arise from a specific part of the brain stem (midbrain, pons or medulla), or from a junction between two parts: Midbrain – the trochlear nerve (IV) comes from the posterior side of the midbrain. It has the longest intracranial length of all the cranial nerves. Midbrain-pontine junction – oculomotor (III). Pons – trigeminal (V). Pontine-medulla junction – abducens, facial, vestibulocochlear (VI-VIII). Medulla Oblongata – posterior to the olive: glossopharyngeal, vagus, accessory (IX-XI). Anterior to the olive: hypoglossal (XII). The cranial nerves are numbered by their loca
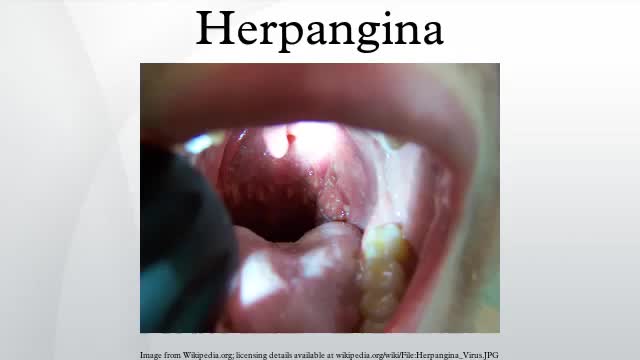
Herpangina is a common childhood illness caused by a virus. It is characterized by small, blister-like ulcers on the roof of the mouth and in the back of the throat. The infection may also cause a sudden fever, sore throat, headache, and neck pain.
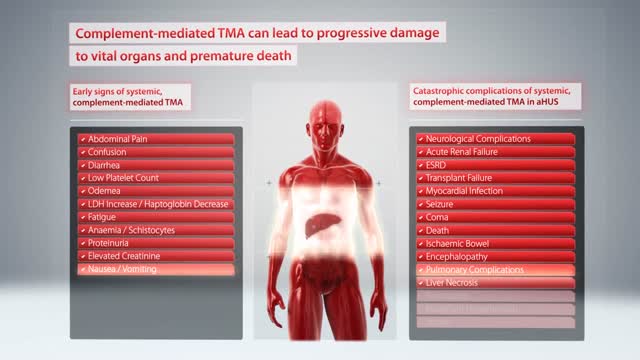
Hemolytic-uremic syndrome (or haemolytic-uraemic syndrome), abbreviated HUS, is a disease characterized by hemolytic anemia (anemia caused by destruction of red blood cells), acute kidney failure (uremia), and a low platelet count (thrombocytopenia).

In cases when the presentation is unclear, ultrasonography is the imaging methodology of choice. The characteristic finding is the presence of a "target sign". Ultrasonography is not required in patients with obvious clinical diagnosis (as seen in this patient). Such patients can proceed directly to treatment with diagnostic and therapeutic air (pneumatic) or water-soluble (hydrostatic contrast) enema.
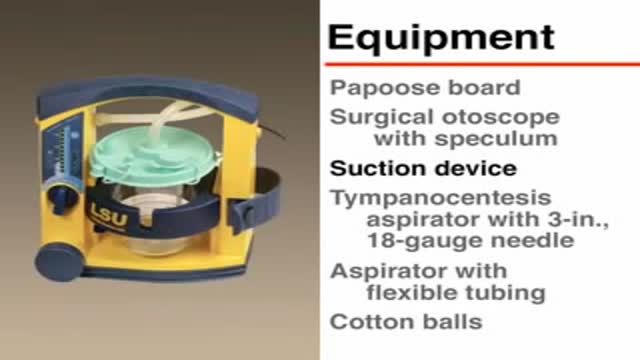
This is a Video in Clinical Medicine from the New England Journal of Medicine. Tympanocentesis in Children with Acute Otitis Media Overview Tympanocentesis is defined as needle aspiration of fluid from the middle ear. In children with acute otitis media, drainage of pus from the middle ear results in a rapid and marked improvement in symptoms and enables the clinician to prescribe tailored antimicrobial therapy. This video will demonstrate the technique of tympanocentesis. Indications Tympanocentesis is recommended in children with refractory acute otitis media, in immunocompromised children with otitis media, and in children with suppurative complications of acute otitis media, . . . .

Body Mass Index (BMI) is a person's weight in kilograms divided by the square of height in meters. A high BMI can be an indicator of high body fatness. BMI can be used to screen for weight categories that may lead to health problems but it is not diagnostic of the body fatness or health of an individual.May 15, 2015
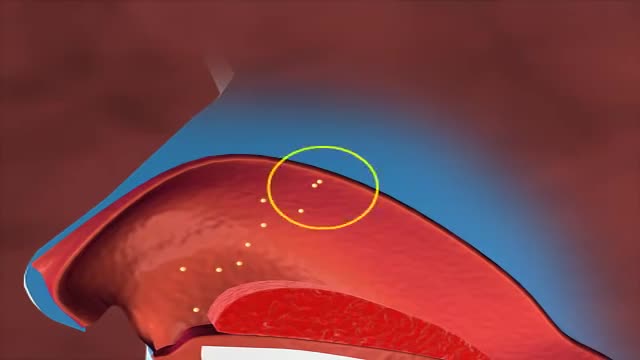
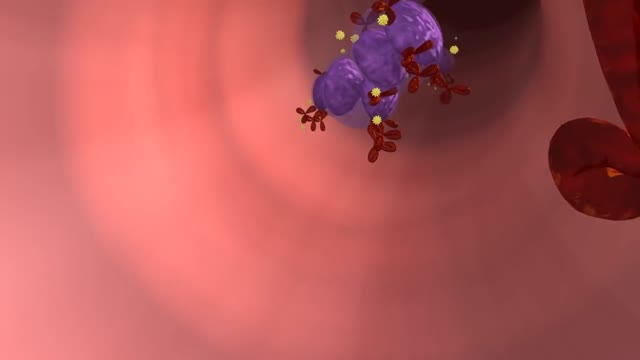
This is a video on allergic mechanism in our body.this animation video shows how allergens come in contact and how does the body react to such allergens and what is the effect of anti histamine drugs over these allergens.
The National Institute of Allergy and Infectious Diseases explains food allergy and offers tips on how to manage the condition.
There is a strong association with obesity. In children younger than 10 years, it is associated with metabolic endocrine disorders {hypothyroidism, panhypopituitarism, hypogonadism, renal osteodystrophy, growth hormone abnormalities). SCFE is considered chronic if it has been present more than 3 weeks and acute if it has been present for 3 weeks or less. It is called "stable" if the patient can bear weight and "unstable" if the patient cannot ambulate. Unstable SCFE is associated with more complications, including avascular necrosis of the femoral head (AVN). SCFE is diagnosed by x-ray of the pelvis and bilateral hips. The underlying cause is a widened epiphyseal growth plate, due to abnormal cartilage maturation and endochondral ossification. The treatment is surgical, requiring immediate internal fixation with a single screw. Delay in treatment {> 24 hours) leads to increased AVN, SCFE progression from stable to unstable, and high risk of future degenerative arthritis. Prophylactic contralateral fixation of the unaffected hip is not routinely done in the U.S., except in patients with endocrine abnormalities.
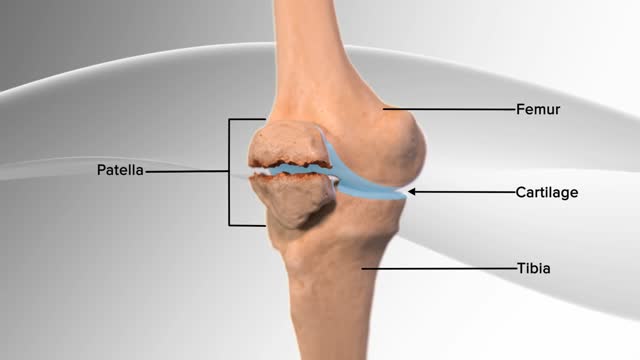
In this knee procedure, the patella is being repaired. The patella is a small, floating bone that glides over the thighbone. It connects the muscles of the thigh to the shinbone, helping the knee to move. The egg‐shell type covering on the underside of the patella and front of the femur allows for smooth motion of the knee.
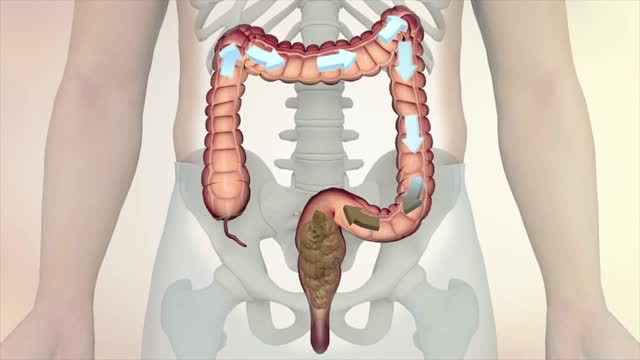
This information is collected from Oncolex. For more on colon and rectum (
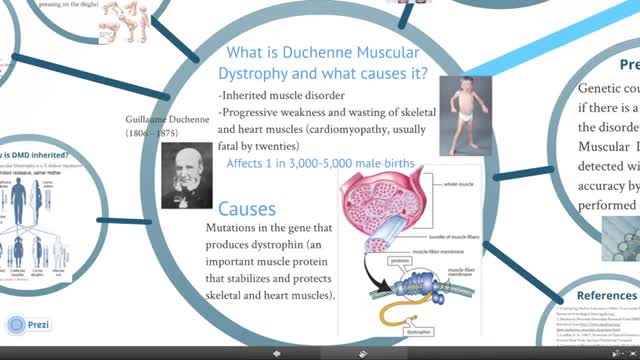
This patient's age, speech delay, bilateral lower-extremity weakness, apparent increase in calf diameter, and history of a wheelchair-bound uncle are typical of Duchenne muscular dystrophy (DMD). DMD is the most common muscular dystrophy of childhood that affects boys who have inherited a defective dystrophin gene on X-chromosome p21. Weakness begins in the proximal lower-extremity muscles and manifests as difficulty walking, running, jumping, and climbing stairs. Boys may push their arms on their thighs (Gower sign) to transition from sitting to standing.

Dental Implant Procedure - Two Stage
