- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Total laparoscopic hysterectomy using staples to secure major blood vessels. Vaginal colpotomy and mobilization of bladder performed initally with suture line at junction of vagina and cervix visualized laparoscopically.
http://crohnsulcerativecolitis.plus101.com/
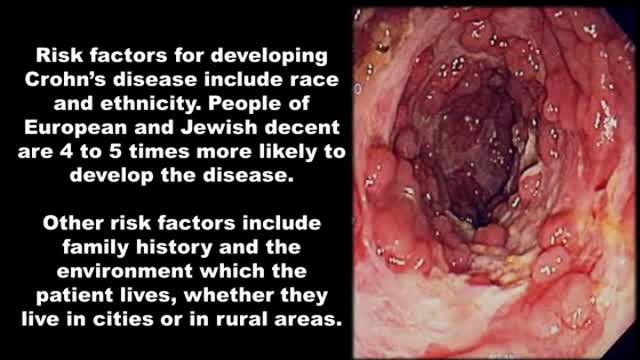
----Crohn's Disease Symptoms Pain. Are you suffering from diarrhea that sometimes leaves you feeling that you've completely emptied your intestine from eveything you've eaten that week?
Have you seen bright red blood traces in your stool or on the toilet paper at least once?
Do you sometimes have abdominal cramps after your meals?
Do you at times feel so nauseous that food doesn't have any appeal to you?
Have you had at least one onset of unexplained low grade fever?
Do you joints sometimes feel itchy, sore or painful?
Did you ever notice red spots or blisters on your arms or legs?
Did you ever experience episodes of itchy and even painfull pink eye (conjuctivitis)?
Have you lost weight?
Do you have episodes of overwhelming fatigue?
Do you experience increased frequency of bowel movement?
Did you ever get up during the night to defecate?
Crohn's, Disease, Symptoms, Pain, symptoms of crohns, chrons disease symptoms , ulcerative colitis symptoms, symptoms of colitis, United States, United Kingdom, Canada, ulcerative colitis diet, ulcerative colitis treatment, irritable bowel symptoms

Colonoscopy Showing Moving Parasites

Watch that video of The Real Human Body Decomposition Process

Baby born without brain
The maneuver is commonly used during some activities: Straining to have a bowel movement Blowing a stuffy nose Certain medical tests or exams As a pressure equalization technique by scuba divers, sky divers and airplane passengers The effect of the Valsalva Maneuver is a drastic increase in the pressure within the thoracic cavity.
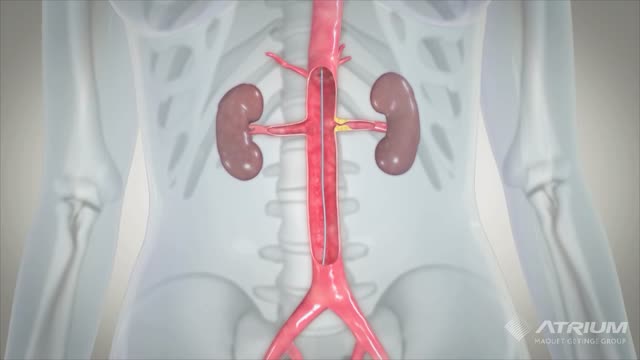
A ureteral stent, sometimes as well called ureteric stent, is a thin tube inserted into the ureter to prevent or treat obstruction of the urine flow from the kidney. The length of the stents used in adult patients varies between 24 to 30 cm.

Giant Swollen Leg Elephantiasis Filariasis

Allergic bronchopulmonary aspergillosis (ABPA) is a condition characterised by an exaggerated response of the immune system (a hypersensitivity response) to the fungus Aspergillus (most commonly Aspergillus fumigatus). It occurs most often in patients with asthma or cystic fibrosis.
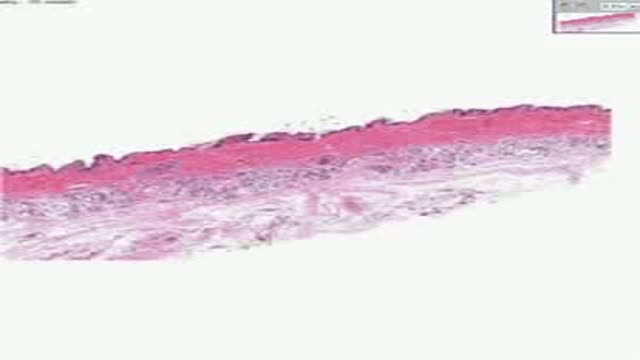
Histology of Skin Appendages

Abortion real ghraphics

Achieving and maintaining long-term weight loss goals.

Galant Reflex

Skin cancer is the most common of all cancer types, accounting for an estimated one third of all new cases. It’s important to take the right steps to ensure proper protection and adopt good sun care habits no matter what your age or stage in life.
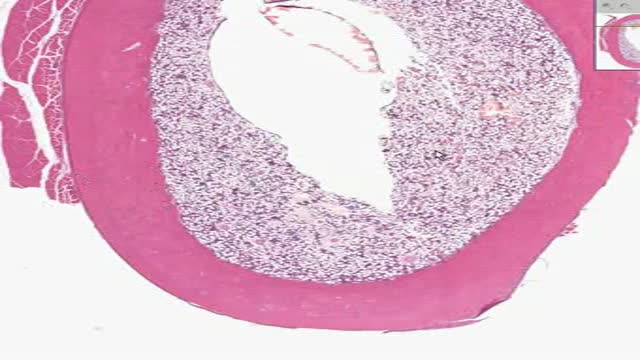
Histology of Dense Bone
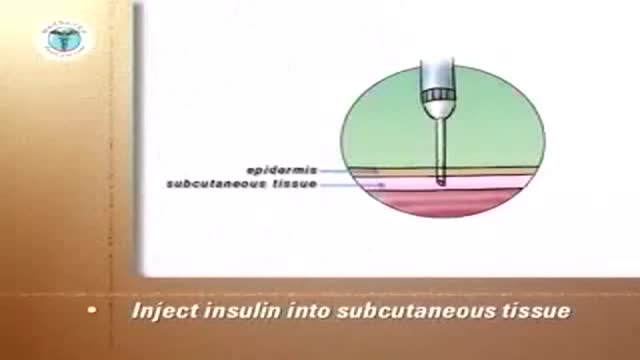
Insulin Pen
MEdRC is a medical elearning company in India.

Hemorrhoidectomy Operation Video

Migraine headaches are recurrent throbbing or pulsatile headaches often associated with a prodrome, nausea, vomiting, photophobia, and phonophobia. When they occur, the prodromes are characterized by visual scintillations, scotomas, dizziness, or tinnitus

Will you still love me if I have herpes? About 1 in 6 Americans between the ages of 14 and 49 is infected with herpes simplex virus type 2, according to a health survey released by the Centers for Disease Control and Prevention. If you’re living with herpes, HSV, HPV or other STDs, you're recommended to check out the largest STD support site STDdatings.
