- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

A c-section, or cesarean section, is the delivery of a baby through a surgical incision in the mother's abdomen and uterus. In some circumstances, a c-section is scheduled in advance. In others, the surgery is needed due to an unforeseen complication. If you or your baby is in imminent danger, you'll have an emergency c-section. Otherwise, it's called an unplanned section. According to the U.S. Centers for Disease Control, about 32 percent of American women who gave birth in 2015 had a cesarean delivery.

An interesting documentary video from Discovery channel from the show "Human Files Night" explaining the anatomy and everything related to female genital tract in a very interesting professional way.

Changing Dressing Wounds

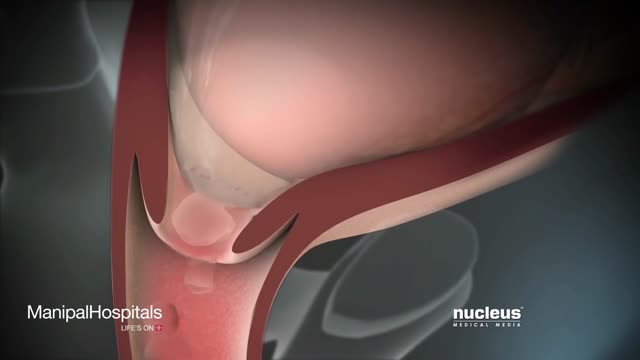
Ptosis is when the upper eyelid droops over the eye. The eyelid may droop just a little, or so much that it covers the pupil (the black dot at the center of your eye that lets light in). Ptosis can limit or even completely block normal vision. Children and adults can have ptosis. Fortunately, this condition can be treated to improve vision as well as appearance.

Shut the front door: Scientists have finally found the perfect breasts. No, they weren't hiding in the Amazon or roving solo across the Sahara (although we have no doubt there are women in both the Amazon and the Sahara who have magnificent mammaries); it turns out these perfect breasts were hiding in a plastic surgeon's office this whole time! Now, before you get all worked up, the American Society of Plastic Surgeons (ASPS) would like you to know that the super-fake looking plastic breasts of yore are not actually what people think are most attractive now. According to a study published in the Journal of Plastic and Reconstructive Surgery—which involved asking over 1,300 people to look at pictures of naked boobies and rank them by hotness (stop laughing, this is serious research!)—people preferred a more "real" and "normal" look from their silicone, with the ideal breast shape having a 45:55 ratio. People said the best chests have 45 percent of the fullness above the nipple line and 55 percent of the fullness below, in a slightly teardrop shape. Researchers noted this preference remained consistent across gender, racial, and ethnic groups with the 45:55 ratio favored by 87 percent of women in their 30s, 90 percent of men, and 94 percent of plastic surgeons.

The Zika virus, first identified in Uganda in 1947, is transmitted by the same type of mosquito that carries dengue fever, yellow fever, and chikungunya virus. A mosquito bites an infected person and then passes those viruses to other people it bites. Outbreaks did not occur outside of Africa until 2007, when it spread to the South Pacific.
What causes rheumatic fever? Rheumatic fever is not an infection itself, but rather the result of an untreated strep infection. When your body senses the strep infection, it sends antibodies to fight it. Sometimes, these antibodies attack the tissues of your joints or heart instead. If the antibodies attack your heart, they can cause your heart valves to swell, which can lead to scarring of the valve "doors" (called leaflets or cusps). Who is at risk for rheumatic fever? Fewer than 0.3% of people who have strep throat also get rheumatic fever. Rheumatic fever is most common among children aged 5 to 15, but adults may have the condition as well. Doctors think that a weakened immune system may make some people more likely to get rheumatic fever. And, although antibiotic medicines have reduced the number of cases of rheumatic fever in developed countries, there are still thousands of reported cases. What are the symptoms of rheumatic fever and how is it diagnosed? Symptoms of rheumatic fever usually begin 1 to 6 weeks after you have had a strep infection. They are Fever Joint pain or swelling in your wrists, elbows, knees, or ankles Small bumps under the skin over your elbows or knees (called nodules) A raised, red rash on your chest, back, or stomach Stomach pain or feeling less hungry Weakness, shortness of breath, or feeling very tired Your doctor will begin by doing a throat culture to find out if you have a strep infection. Then, your doctor will use a stethoscope to listen to your heart. He or she will also look for nodules on your joints. Sometimes, blood tests, chest x-rays, or an electrocardiogram (ECG or EKG) may be needed for a more definite diagnosis. How is rheumatic fever treated? Rheumatic fever must be treated right away. If you have a sore throat that lasts longer than 3 days, or if you have a fever and headache along with your sore throat, you should see your doctor for a throat culture. Even if you do not have a sore throat but have a fever and a skin rash, this could also mean a strep infection, and you should get tested. Remember rheumatic fever can result from an untreated strep infection, so it is very important to treat the infection before it leads to a worse condition.

Get the facts and fight back against Dry Eye disease.
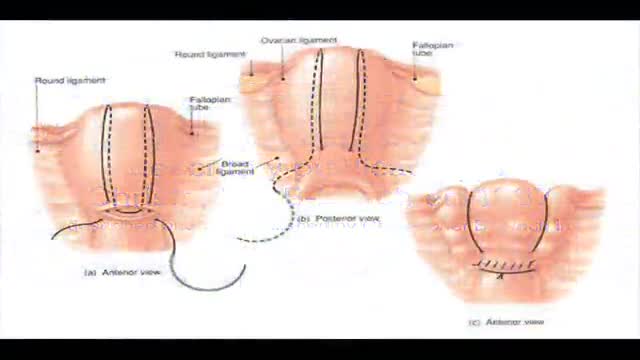
B-Lynch suture for uterine atony technique described

this video shows how the child circumcision is easy and safe with alisklamp
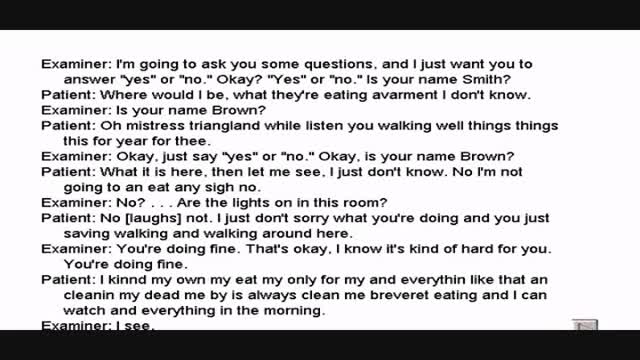
Wernicke's aphasia is a neurological disorder typically caused by stroke. It affects the Wernicke's region in the brain's left hemisphere which is reasoned to be responsible for processing of meaning, especially as it relates to verbal communication, hence the problems with speech witnessed in these patients

Pediatric Urine Samples Collection
Labor And Delivery During Vaginal Child Birth
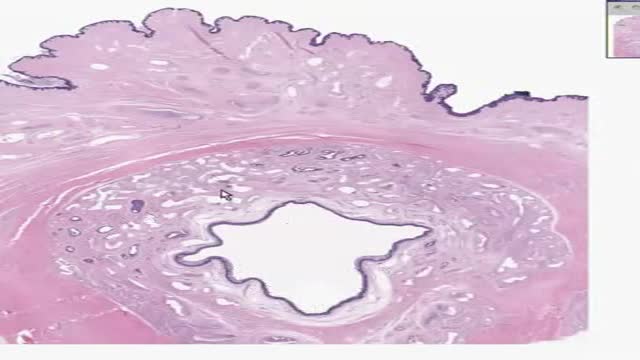
Histology of Male Urethra

Routine Pap Smear and Pelvis Exam For Canadian Women

This condition is seen in imperforate hymen or transverse vaginal septum. Pt presents with primary amenorrhea. Dr Hemant Damle Prof Dept of OBGYN SKNMC Pune India
A report of Female Genital Mutilationn FGM (female circucision) in Menya In Egypt تقرير من مدينة المنيا في صعيد مصر عن ختان لاناث
http://www.vaginal-ultrasound.com A demonstration of a vaginal ultrasound.
Detroit Medical Center video on Bariatric surgery for diabetes patients. ~ Detroit Medical Center

Female Circumcision - FGM Female Genital Mutilation - female circumcision ختان الاناث - женское обрезание - circuncisão feminina - 女性割禮 - besnijdenis - babae pagtutuli - l'excision - κλειτοριδεκτομή - הנקבה מולה - sunat perempuan - circoncisione femminile - 女子割礼 - 여성 할례 - la circuncisión femenina - หญิง circumcision - kadın sünnet - жіноче обрізання For More read at World Health Organization web site : http://www.who.int/topics/female_genital_mutilation/en/index.html other sites : http://en.wikipedia.org/wiki/Female_genital_cutting
