Top video's
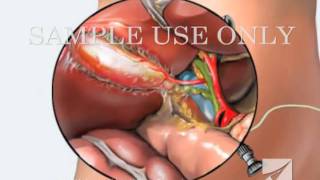
This medical animation shows laparoscopically assisted gallbladder removal surgery, or cholecystectomy. The animation begins by showing the normal anatomy of the liver and gallbladder. Over time, gallstones form within the gallbladder, blocking the cystic duct, and causing the gallbladder to become enlarged and inflamed. The procedure, sometimes called a "lap-chole", begins with the insertion of four trocar devices, which allow the physician to see inside the abdomen without making a large incision. Air is added to the abdominal cavity to make it easier to see the gall bladder. Next, we see a view through the laparascope, showing two surgical instruments grasping the gallbladder while a third severs the cystic duct. After the gallbladder is removed, the camera pans around to show that the cystic artery and vein, have already been clipped to prevent bleeding.
Item #ANIM026

This surgical animation is for patient education and describes a laparoscopic colectomy, which is a type of minimally invasive surgery for colon cancer. Laparoscopic colectomy, also called minimally invasive colectomy, involves several small incisions in your abdomen. Instead of a big incision, the surgeon makes a few small cuts (0.5-1 centimeters) in the abdominal cavity to insert a surgical camera and instruments and perform the operation. A slightly bigger incision, about 3.5 centimeters wide, is made to remove the tumor.
When compared to traditional open surgery, laparoscopic colectomy can result in much less pain and swifter recovery. Depending on the procedure, most laparoscopic colectomy patients leave the hospital and return to normal activities more quickly than patients recovering from open surgery.
Colorectal cancer is the second leading cause of cancer death in the United States.
For more information about 3d animation videos, please visit https://www.amerra.com

VirtaMed's new laparoscopy simulator starts with patient safety.
VirtaMed LaparoS™
-Starts at the beginning and covers crucial procedure preparation steps
- Innovative skills training derived from validated concepts
- Start with patient safety: abdomen positioning and trocar placement
- Covers crucial procedure preparation steps
Numerous medical training institutions have found that integrating simulation into their curriculum both improves training outcomes and ultimately supports better patient care. Benefit from VirtaMed’s decades of experience and expertise in laparoscopy training and education.

This video demonstrate Bilateral Salpingectomy for a patient suffering from hematosalpinx of one side and Hydrosalpinx other side in which one IVF has failed. Laparoscopic salpingectomy. In this less-invasive procedure, the surgeon makes 1-3 small incisions in the lower abdomen, and inserts a laparoscope into the pelvis through one of the incisions. The camera at the end of the laparoscope guides the surgeon through the procedure. The fallopian tube tissue is then removed. For more information https://www.laparoscopyhospital.com/
For more information please contact:
World Laparoscopy Hospital
Cyber City, Gurugram, NCR DELHI
INDIA 122002
Phone & WhatsApp: +919811416838, + 91 9999677788

Dr. Lohith U, Consultant Surgical Gastroenterology, Bariatric and GI Oncology, Manipal Hospital Sarjapur, speaks about advanced laparoscopic surgery in this informative video. He shares details about the procedure,insights on its advantages, and how it can help treat gastrointestinal issues without making large incisions in a patient’s body. To know more watch this video.
Consult the experts here - https://bit.ly/3RiWqPr
#ManipalHospitalSarjapur #YourManipal #LifesOn #Healthcare #LaparoscopicSurgery

What to expect during the day of a pediatric surgery at Sutter Children's Center Sacramento.

Dr. Fizan Abdullah is head of the Division of Pediatric Surgery and vice chair of the Department of Surgery at Ann & Robert H. Lurie Children's Hospital of Chicago. His special interests include Chest wall deformities, pectus excavatum, abdominal wall defects, neonatal surgery, pulmonary and upper airway malformations, congenital diaphragmatic hernia, esophageal and gastrointestinal anomalies, hernia repair, tissue engineering, extracorporeal membrane oxygenation (ECMO), surgical safety protocols and surgical infections.
Learn more at www.luriechildrens.org

If you have an upcoming procedure at UC Davis Children’s Surgery Center, this video provides information and details of what you and your family can expect from arrival to check-in through to surgery and after care.
This video is also available in these languages:
Arabic: https://youtu.be/ERPikb0prlI
Dari: https://youtu.be/UW5fT433IGQ
Punjabi: https://youtu.be/Xq6PV2qtOMo
Russian: https://youtu.be/v223nDdN1b4
Spanish: https://youtu.be/4Jr4dkzAaWA
——
At UC Davis Children’s Hospital, we put your child at the center of everything that we do. It’s personalized care, uniquely sized for your child. You’ll see it in our child-friendly designs throughout the hospital, our farm-to-fork approach to dining, our playrooms and teen rooms and our team that feels like family. UC Davis Children’s Hospital is Sacramento’s only nationally ranked, comprehensive hospital for children, serving infants, children, adolescents and young adults with primary, subspecialty and critical care.
UC Davis Children’s Hospital: https://children.ucdavis.edu
Children’s Surgery Center: https://health.ucdavis.edu/chi....ldren/services/child
Child Life and Creative Arts Therapy: https://health.ucdavis.edu/chi....ldren/services/child
Fetal Care and Treatment Center: https://health.ucdavis.edu/chi....ldren/services/fetal
See the latest news from UC Davis Health: https://health.ucdavis.edu/newsroom
Kids Considered podcast: https://www.youtube.com/playli....st?list=PLM7qvIv8N9R
Facebook: https://www.facebook.com/UCDavisChildrensHospital
Instagram: https://www.instagram.com/ucdavischildren
Twitter/X: https://twitter.com/UCDavisChildren
——
#surgery #childrenshospital #surgeryrecovery #ucdavis
How did Mr Bean get himself into pretending to be a doctor?

Dr. Ailawadi, M.D., the Chair of Cardiac Surgery at Michigan Medicine, specializes in minimally invasive valve surgery as well as complex cardiac operations. This video shows step by step footage of a Coronary Artery Bypass Graft (CABG) in a complex patient. In this case, CABG was performed through a sternotomy (through the breast bone) using the internal thoracic artery and saphenous leg veins to bypass obstructed coronary arteries. In this video, Dr. Ailawadi will perform a triple vessel bypass (CABG) which has been shown to minimize the risk of future heart attack and help patients live longer in the setting of complex coronary artery disease.
To learn more about cardiac surgery at Michigan Medicine, visit: https://medicine.umich.edu/dept/cardiac-surgery
To learn more about Frankel Cardiovascular Center, visit: https://www.umcvc.org/
To watch the full playlist, visit: https://www.youtube.com/playli....st?list=PLNxqP-XbH8B
-------------------------------------------------------
Subscribe to Michigan Medicine’s YouTube channel for upcoming videos and future live streams featuring our experts answering your questions.
-------------------------------------------------------
Follow Michigan Medicine on Social:
Twitter: https://twitter.com/umichmedicine
Instagram: https://www.instagram.com/umichmedicine/
Facebook: https://www.facebook.com/MichiganMedicine/
Follow the U-M Frankel Cardiovascular Center on Social:
Twitter: https://twitter.com/umichcvc
Facebook: https://www.facebook.com/Unive....rsityofMichiganCardi
#MichiganMedicine #MedEd #CardiacSurgery #UniversityOfMichiganHealth #FrankelCardiovascularCenter #Cardiology #CardiacSurgeon

Dr. Joanna Chikwe, explains how patients may feel after heart surgery.
Learn more about the Smidt Heart Institute at Cedars-Sinai at https://ceda.rs/3meIA2A
Learn more about Dr. Joanna Chikwe at https://ceda.rs/3ul6I6t
Connect with us:
https://twitter.com/CedarsSinai
https://www.facebook.com/CedarsSinai
https://www.instagram.com/CedarsSinai
Cedars-Sinai is a leader in providing high-quality healthcare encompassing primary care, specialized medicine and research. Since 1902, Cedars-Sinai has evolved to meet the needs of one of the most diverse regions in the nation, setting standards in quality and innovative patient care, research, teaching and community service. Today, Cedars- Sinai is known for its national leadership in transforming healthcare for the benefit of patients. Cedars-Sinai impacts the future of healthcare by developing new approaches to treatment and educating tomorrow’s health professionals. Additionally, Cedars-Sinai demonstrates a commitment to the community through programs that improve the health of its most vulnerable residents.

Ever wanted to see an open heart surgery? Dr. Sandwith, the only open-heart surgeon in the tri-county area, takes you into the OR to improve the life of a gentlemen with congenital heart disease.
#HCA_FL #FortWaltonDestinHospital

Emory has one of the few heart and vascular centers nationally performing robotic cardiac surgery using the daVinci Surgical System. Emory's robotic surgeons have completed numerous cases and are recognized in Atlanta, the Southeast and across the country for their expertise in cardiac surgery. Some of the cardiac and thoracic conditions treated by Emory cardiac surgeons include mitral valve repair and replacement, atrial septal defect repair, atrial myxoma and thrombi, coronary bypass (LIMA to LAD), mediastinal mass excision, thymectomy, epicardial lead placement and pericardial window.

To learn more about coronary artery bypass grafting (CABG), please visit https://cle.clinic/3b7dqpE
Cardiac surgeons Faisal Baaeen, MD and Edward Soltesz, MD talk about coronary artery bypass graft (CABG) surgery in this informative video.
They describe:
• how blockages are bypassed
• how vessels are used for the bypass graft
• reoperation experiences
• the importance of complete revascularization
• and options such as off pump bypass surgery and minimally invasive surgery
Dr. Bakaeen is the Director of the Coronary Artery Bypass Center at Cleveland Clinic. To learn more about him, please visit https://cle.clinic/2INN9AV
Dr. Soltesz is a cardiovascular and heart transplant surgeon. To learn more about him, please visit https://cle.clinic/3o86RMt
▶Share this video with others: https://youtu.be/Cp59BCMVHHc
▶Subscribe to learn more about @clevelandclinic
#clevelandclinic #coronaryartery #bypasssurgery #heartsurgery #heartcare #cardiacsurgery
► Get a free NCLEX NGN sample test today: http://lectur.io/nclexrnsampletestyt
► Create your free account today: http://lectur.io/nurseregisteryt
► If you’re an nursing educator or faculty member, visit: http://lectur.io/nursytb2u
Want to know more about Clinical Skills?
Start watching our Clinical Skills course: http://lectur.io/fundamentalsclinical...
Lecturio is your smart tutor for nursing school: Learn the toughest NCLEX® topics with high-yield video lectures, integrated quiz questions, and more. Join Lecturio Nursing now: http://lectur.io/mg1
► INSTALL the free Lecturio app
iTunes Store: https://app.adjust.com/z21zrf
Play Store: https://app.adjust.com/b01fak
► CHECK OUT ALL NURSING COURSES:
Leadership Nursing: http://lectur.io/leadershipnursing
Dosage Calculation Nursing: http://lectur.io/dosagecalcnursing
Physiology Nursing: http://lectur.io/physiologynursing
Medical Surgical Nursing: http://lectur.io/medsurgnursing
Pharmacology Nursing: http://lectur.io/pharmacologynursing
NCLEX® Pharmacology Nursing: http://lectur.io/pharmnclexnursing
Pediatric Nursing: http://lectur.io/pediatricnursing
Study Skills Nursing: http://lectur.io/studyskillsnursing
Fundamentals of Nursing - Theory: http://lectur.io/fundamentalstheory
Fundamentals of Nursing - Clinical Skills: http://lectur.io/fundamentalsclinical...
Nursing Prerequisites: http://lectur.io/nursingprerequisites
Mental Health Nursing: http://lectur.io/mentalhealthnursing
Nursing Care of Childbearing Family: http://lectur.io/maternalnewbornnursing
► SUBSCRIBE to our YouTube channel: http://lectur.io/subscribenursing
► WATCH MORE ON YOUTUBE: http://lectur.io/nursingplaylists
► LET’S CONNECT:
Facebook: www.facebook.com/lecturio.nursing
Instagram: www.instagram.com/lecturio_nursing
TikTok: www.tiktok.com/@lecturio_nursing
LinkedIn: https://www.linkedin.com/company/lecturio-medical/
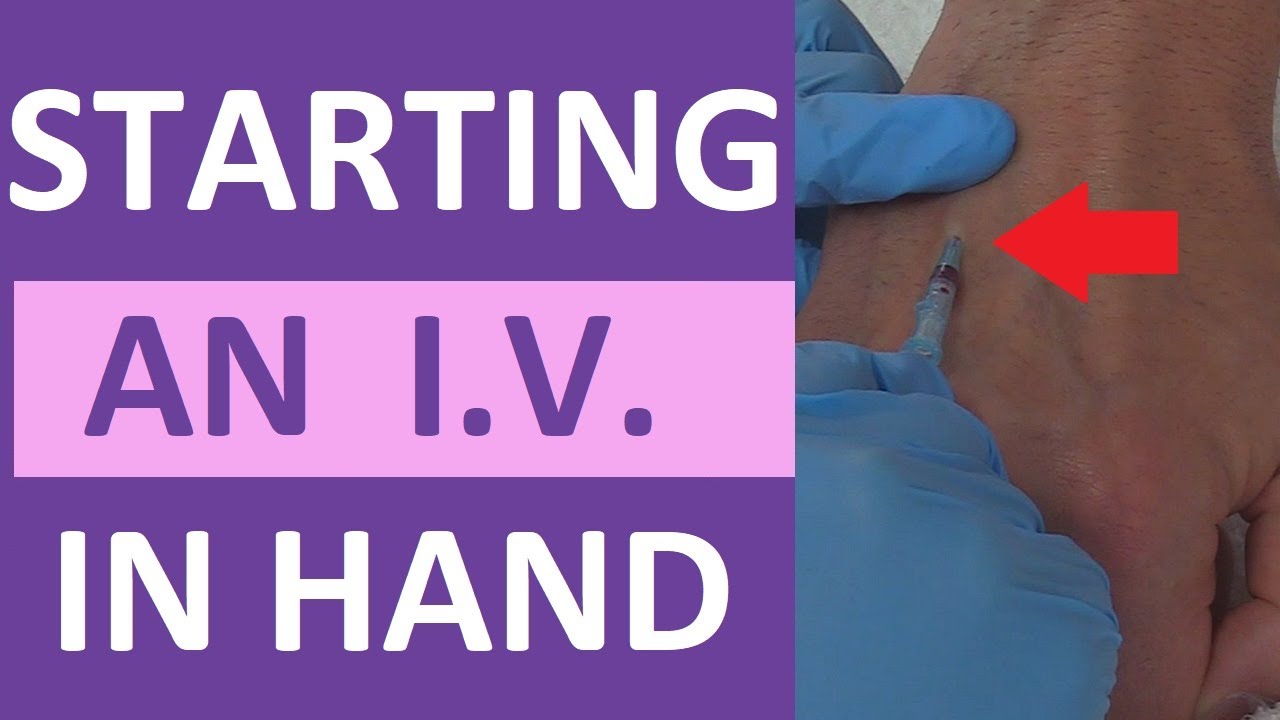
How to start a peripheral IV in the dorsum of the hand: clinical nursing skill technique.
Starting an IV (intravenous catheter) can be an intimidating experience for nurses, especially nursing students and new nurses. However, nurses will perform IV insertions often, so this is an important nursing skill to learn.
Before starting an IV, always follow the protocols of your facility, as well as manufacturer's instructions for any supplies used.
In this video, Nurse Sarah demonstrates how to start a peripheral IV in the dorsum of the hand. Prior to inserting the IV, you'll want to do the following:
-Gather supplies
-Perform hand hygiene
-Prepare supplies (including priming the saline flush, removing air from extension tubing, opening packages, completing labels, and any other steps required by your facility.
-Locate a suitable vein
-Perform hand hygiene
-Don gloves
If the patient has a lot of hair, you might want to use clippers to trim the hairs prior to starting the IV. You may also apply a tourniquet to help veins move near the surface of the skin.
Next, you'll want to clean the site using the cleaner that came in the IV start kit, such as ChloraPrep.
Once the site has dried completely, you can insert the IV. Stabilize the vein with your non-dominant hand, and insert the IV's needle into the vein, watching carefully for blood return (or a blood flash) in the chamber. Advance the IV around 2mm more to ensure the plastic cannula is in the vein, then thread the cannula into the vein and press the needle safety button.
Notes: https://www.registerednursern.....com/how-to-start-an-
IV Video Series: https://www.youtube.com/watch?v=MbG_1-_mnoo&list=PLQrdx7rRsKfXr6kruqEpIovf66sxo0gxh
This video also demonstrates how to flush the IV using the push-pause method, how to secure the IV using the Tegaderm dressing that came with the IV start kit, considerations of the different cap types and the clamp sequence, and more.
For more information, watch the complete tutorial.
#nurse #nursing #iv #startiv #ivtherapy
Website: https://www.registerednursern.com/
More Videos: https://www.youtube.com/watch?v=R2XMro13dD0&list=UUPyMN8DzkFl2__xnTEiGZ1w
Nursing Gear: https://teespring.com/stores/registerednursern
Instagram: https://www.instagram.com/registerednursern_com/
Facebook: https://www.facebook.com/RegisteredNurseRNs
Twitter: https://twitter.com/NursesRN
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf

The head-to-toe assessment in nursing is an important physical health assessment that you'll be performing as a nursing student and nurse.
Head-to-toe assessments allow nurses to assess the health status of patients by following a checklist of criteria.
On the job, your head-to-toe nursing assessment will be performed much faster, and it may be different or more specialized to accommodate the patients' needs within your nursing specialty.
This assessment represents a general assessment checklist (or cheat sheet) that you might encounter in nursing school. (Note: Always follow your instructor's requirements or your employer's assessment protocols).
This nursing head-to-toe examination video guide will focus on the following areas/skills:
-Vital Signs (pulse rate, respiration rate, temperature, oxygen saturation, blood pressure, pain assessment)
https://www.youtube.com/watch?v=gUWJ-6nL5-8
-Cranial Nerve examination
-Head assessment (hair, cranium, eyes, nose, mouth, ears, sinuses)
-Neck assessment (jugular vein, thyroid, trachea, carotid)
-Heart sounds assessment: https://www.youtube.com/watch?v=H48WsyIjFs0&t=73s
-Lung sounds assessment: https://www.youtube.com/watch?v=KNrcG077brQ
-Abdominal assessment
-Assessing extremities (arms, hands, legs, feet)
-Back assessment
-and more
While performing your comprehensive head-to-toe assessment, you'll want to record your findings in the documentation.
Nursing Gear: https://teespring.com/stores/registerednursern
Subscribe: http://www.youtube.com/subscri....ption_center?add_use
Notes: http://www.registerednursern.c....om/head-toe-assessme
Nursing School Supplies: http://www.registerednursern.c....om/the-ultimate-list
Visit our website RegisteredNurseRN.com for free quizzes, nursing care plans, salary information, job search, and much more: http://www.registerednursern.com
Check out other Videos: https://www.youtube.com/user/R....egisteredNurseRN/vid
All of our videos in a playlist: https://www.youtube.com/watch?v=pAhHxt663pU&list=PLQrdx7rRsKfXMveRcN4df0bad3ugEaQnk
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing School Study Tips: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing School Tips & Questions" https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Teaching Tutorials: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Types of Nursing Specialties: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Healthcare Salary Information: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
New Nurse Tips: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Career Help: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
EKG Teaching Tutorials: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Dosage & Calculations for Nurses: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Diabetes Health Managment: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf

WATCH MORE NURSING SKILLS HERE: https://nursing.com/course/nursing-skills/?utm_source=youtube&utm_medium=social
In our Nursing Skills course, we show you the most common and most important skills you will use as a nurse! We included everything from bed baths, to inserting a foley, to advanced skills like chest tube management.
Welcome to the NURSING Family, we call it the most supportive nursing cohort on the planet.
At NURSING.com, we want to help you remove the stress and overwhelm of nursing school so that you can focus on becoming an amazing nurse.
Check out our freebies and learn more at: (http://www.nursing.com)
Visit us at http://www.nursing.com/medical....-information-disclai for disclaimer information.
NCLEX®, NCLEX-RN® are registered trademarks of the National Council of State Boards of Nursing, INC. and hold no affiliation with NURSING.

► Get a free NCLEX NGN sample test today: http://lectur.io/nclexrnsampletestyt
► Create your free account today: http://lectur.io/nurseregisteryt
► If you’re an nursing educator or faculty member, visit: http://lectur.io/nursytb2u
In this video “How To Do An IM (Intramuscular) Injection” you will learn about:
►the steps in the administration of intramuscular medications
►the angle to position the syringe while administering an intramuscular injection
►the landmark to administer an intramuscular injection in the deltoid muscle
►5 tips for the safe administration of an intramuscular medication
►the steps of the Z-track method for intramuscular injections
►the role of aspirating blood during an intramuscular injection and evaluate whether this practice is currently in use
► This video is part of the Lecturio course “Fundamentals of Nursing: Clinical Skills”
► WATCH the complete course on http://lectur.io/njection
► THE PROF: Samantha Rhea MSN, RN has been a nurse since 2008 and a nursing faculty teacher since 2012. She has been recognized for clinical excellence as an interventional cardiology nurse and also led a Joint Commission Accredited Stroke Center. Ms. Rhea is an award-winning expert in clinical teaching and continues to maintain a current clinical practice and teaches at a University nursing program.
► LECTURIO is your smart tutor for nursing school: Learn the toughest NCLEX® topics with high-yield video lectures, integrated quiz questions, and more. Register now to study anytime and anywhere you want to: https://nursing.lecturio.com/#/
► CHECK OUT ALL NURSING COURSES:
Leadership Nursing: http://lectur.io/leadershipnursing
Dosage Calculation Nursing: http://lectur.io/dosagecalcnursing
Physiology Nursing: http://lectur.io/physiologynursing
Medical Surgical Nursing: http://lectur.io/medsurgnursing
Pharmacology Nursing: http://lectur.io/pharmacologynursing
NCLEX® Pharmacology Nursing: http://lectur.io/pharmnclexnursing
Pediatric Nursing: http://lectur.io/pediatricnursing
Study Skills Nursing: http://lectur.io/studyskillsnursing
Fundamentals of Nursing - Theory: http://lectur.io/fundamentalstheory
Fundamentals of Nursing - Clinical Skills: http://lectur.io/fundamentalsclinicalskills
Nursing Prerequisites: http://lectur.io/nursingprerequisites
Mental Health Nursing: http://lectur.io/mentalhealthnursing
Maternal-Newborn Nursing: http://lectur.io/maternalnewbornnursing
► INSTALL the free Lecturio app
iTunes Store: https://app.adjust.com/z21zrf
Play Store: https://app.adjust.com/b01fak
► SUBSCRIBE to our YouTube channel: http://lectur.io/subscribenursing
► WATCH MORE ON YOUTUBE: http://lectur.io/nursingplaylists
► LET’S CONNECT:
Facebook: www.facebook.com/lecturio.nursing
Instagram: www.instagram.com/lecturio_nursing
Join Discord Community: https://discord.gg/Ue95WDxCrp
TikTok: www.tiktok.com/@lecturio_nursing
LinkedIn: https://www.linkedin.com/company/lecturio-medical/
#nursingschool #nursingeducation #nursingclinicalskills #leadershipnursing #nclex #nursingfundamentals #nursingclinical #nursingskills

Hand hygiene for healthcare workers: Learn how to perform hand washing with soap and water (nursing procedures).
There are two ways to perform hand hygiene as a nurse. You can use soap and water or an alcohol-based hand rub (also called hand sanitizer or hand gel).
Hand hygiene is essential for providing safe patient care. If hand hygiene is not performed regularly, germs can be easily be spread to patients, other healthcare workers, and even yourself.
Hand hygiene is ALWAYS performed before and after patient care, after coming into contact with any type of body fluid or open wounds, when touching any object that is near a patient (hand railing, bedside table etc.), removing gloves, prior to eating, or after using the bathroom.
This video discusses when you should use soap and water versus an alcohol-based hand gel, when to perform hand hygiene, and demonstrates how to perform hand hygiene using soap and water.
Notes: https://www.registerednursern.....com/how-to-perform-h
More nursing skills: https://www.youtube.com/watch?v=DBHnd3N-5Ns&list=PLQrdx7rRsKfUhd_qQYEbp0Eab3uUKhgKb
Facebook: https://www.facebook.com/RegisteredNurseRNs
Instagram: https://www.instagram.com/registerednursern_com/
Twitter: https://twitter.com/NursesRN
#handhygiene #handwashing #nursingskills
Subscribe: http://www.youtube.com/subscri....ption_center?add_use
Nursing School Supplies: https://www.registerednursern.....com/the-ultimate-lis
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing School Study Tips: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing School Tips & Questions" https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Teaching Tutorials: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Types of Nursing Specialties: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Healthcare Salary Information: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
New Nurse Tips: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Career Help: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
EKG Teaching Tutorials: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Dosage & Calculations for Nurses: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Diabetes Health Managment: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
