- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

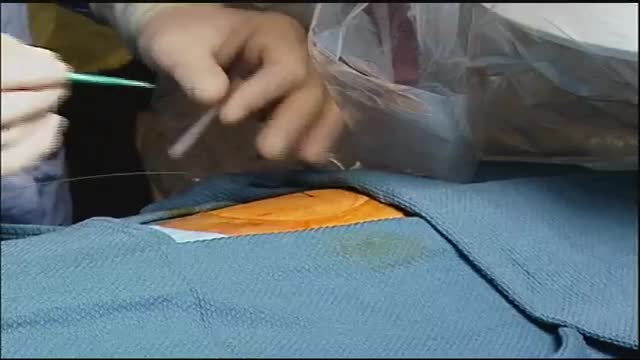
Demonstration of the technique used to insert a drain using an air knot in the operating room.

Conjoined twins Alex and Angel Mendoza from Phoenix, Ariz. were successfully separated after more than 12 hours in surgery, reports Dr. Debbye Turner Bell.

A Medical Video showing an overview of the endocrine and gland system of the human body


Sporotrichosis (also known as "rose gardener's disease") is a disease caused by the infection of the fungus Sporothrix schenckii. This fungal disease usually affects the skin, although other rare forms can affect the lungs, joints, bones, and even the brain.

Vocal Cord Surgery HD
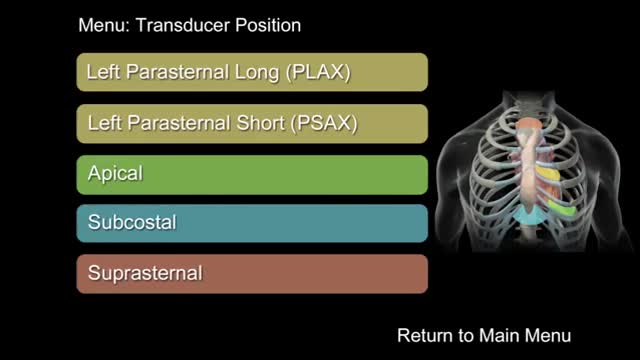
"How to Perform a Transthoracic Echocardiographic Study Volume 1: Transducer Position and Anatomy" is an instructional video, offered by ASE, and can be used for professional lectures and offers an interactive section for flexible presentations. The video includes an overview of relevant cardiac anatomy, a step by step presentation of all Transducer Positions, and the sequential transducer movements to acquire standard echo images needed to complete a Transthoracic Echocardiographic Study.
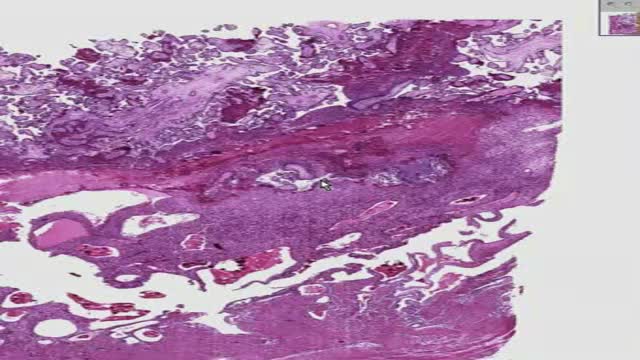
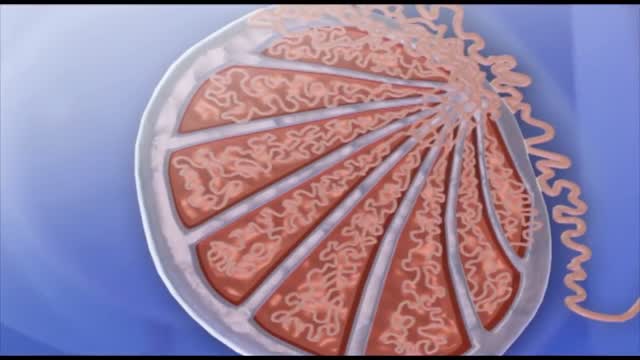
Histology of Placenta
An intra-aortic balloon pump (IABP) is a mechanical device that helps the heart pump blood. This device is inserted into the aorta, the body's largest artery. It is a long, thin tube called a catheter with a balloon on the end of it. If you are hospitalized, your doctor may insert an IABP.
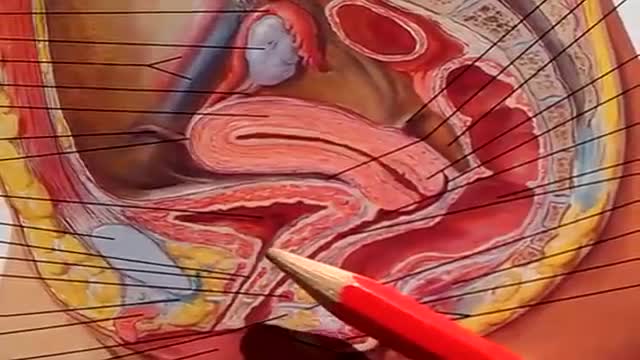
The urinary bladder is a hollow muscular organ that collects urine from the kidneys before disposal by urination. A hollow muscular, and distensible (or elastic) organ, the bladder sits on the pelvic floor. Urine enters the bladder via the ureters and exits via the urethra.
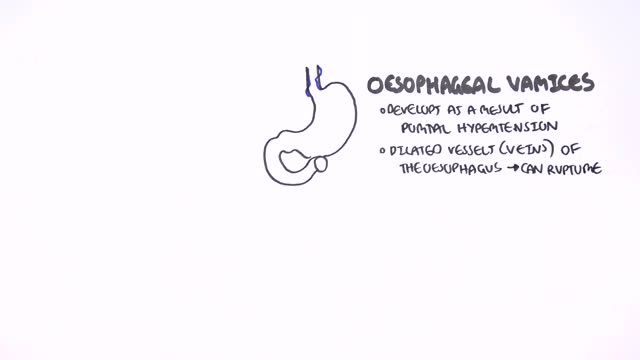
This could be caused by an infection, food poisoning, parasites, Crohn's disease, or reduced blood flow in the colon. Hemorrhoids are another common cause of GI or rectal bleeding. A hemorrhoid is an enlarged vein in your rectum or anus. These enlarged veins can rupture and bleed, causing rectal bleeding.
Pruritis is itchy skin that makes you want to scratch. It can be caused by many things. Normally, itchy skin isn't serious, but it can make you uncomfortable. Sometimes, itchy skin is caused by a serious medical condition. It can occur in association with a primary rash (e.g. dermatitis) or may occur because of hypersensitive nerves in the skin (neuropathic pruritus). ... Scratching a localised itch may lead to lichen simplex, prurigo or prurigo nodularis. Systemic causes of pruritus. Sytemic diseases may cause generalised pruritus.

GIANT EAR WAX REMOVAL By using the elephant ear device.It's very useful video for medical students.Please share it!
Spermatogenesis is the process in which spermatozoa are produced from spermatogonial stem cells by way of mitosis and meiosis. The initial cells in this pathway are called spermatogonia, which yield primary spermatocytes by mitosis.

Bariatric surgical procedures cause weight loss by restricting the amount of food the stomach can hold, causing malabsorption of nutrients, or by a combination of both gastric restriction and malabsorption. Bariatric procedures also often cause hormonal changes. Most weight loss surgeries today are performed using minimally invasive techniques (laparoscopic surgery). The most common bariatric surgery procedures are gastric bypass, sleeve gastrectomy, adjustable gastric band, and biliopancreatic diversion with duodenal switch. Each surgery has its own advantages and disadvantages.

6 987 24 MORE How Does Anesthesia Work? Credit: itsmejust | Shutterstock If you’ve ever had surgery, unless you are super tough, you’ve gone through it with the benefit of anesthetics. But, how do these body-numbing elixirs work? Prior to the invention of anesthesia in the mid-1800s, surgeons had to hack off limbs, sew up wounds and remove mysterious growths with nothing to dull the patient's pain but opium or booze. While these drugs may have numbed the patient, they didn’t always completely block the pain, or erase the memory of it. Since then, doctors have gotten much better at putting us out with drug combinations that ease pain, relax muscles and, in some cases, put us in a deep state of hypnosis that gives us temporary amnesia. Today, there are two primary types of anesthesia drugs: those that knockout the whole body (general) and those that only numb things up locally.

During open-heart valve surgery, the doctor makes a large incision in the chest. Blood is circulated outside of the body through a machine to add oxygen to it (cardiopulmonary bypass or heart-lung machine). The heart may be cooled to slow or stop the heartbeat so that the heart is protected from damage while surgery is done to replace the valve with an artificial valve. The artificial valve might be mechanical (made of man-made substances). Others are made out of animal tissue, often from a pig.
Chorionic villus sampling, often referred to as CVS, is a diagnostic test for identifying chromosome abnormalities and other inherited disorders. This test may be recommended by your health care provider, if you or your partner has family medical histories that reveal potential risks.

Watch that video to know How Hot Dogs are Made
Initially, lead poisoning can be hard to detect — even people who seem healthy can have high blood levels of lead. Signs and symptoms usually don't appear until dangerous amounts have accumulated. Lead poisoning symptoms in children Signs and symptoms of lead poisoning in children include: Developmental delay Learning difficulties Irritability Loss of appetite Weight loss Sluggishness and fatigue Abdominal pain Vomiting Constipation Hearing loss Seizures Eating things, such as paint chips, that aren't food (pica) Lead poisoning symptoms in newborns Babies exposed to lead before birth might: Be born prematurely Have lower birth weight Have slowed growth Lead poisoning symptoms in adults Although children are primarily at risk, lead poisoning is also dangerous for adults. Signs and symptoms in adults might include: High blood pressure Joint and muscle pain Difficulties with memory or concentration Headache Abdominal pain Mood disorders Reduced sperm count and abnormal sperm Miscarriage, stillbirth or premature birth in pregnant women Causes Lead is a metal that occurs naturally in the earth's crust, but human activity — mining, burning fossil fuels and manufacturing — has caused it to become more widespread. Lead was also once used in paint and gasoline and is still used in batteries, solder, pipes, pottery, roofing materials and some cosmetics. Lead in paint Lead-based paints for homes, children's toys and household furniture have been banned in the United States since 1978. But lead-based paint is still on walls and woodwork in many older homes and apartments. Most lead poisoning in children results from eating chips of deteriorating lead-based paint. Water pipes and imported canned goods Lead pipes, brass plumbing fixtures and copper pipes soldered with lead can release lead particles into tap water. Lead solder in food cans, banned in the United States, is still used in some countries. Other sources of lead exposure Lead sometimes can also be found in: Soil. Lead particles from leaded gasoline or paint settle on soil and can last years. Lead-contaminated soil is still a major problem around highways and in some urban settings. Some soil close to walls of older houses contains lead. Household dust. Household dust can contain lead from lead paint chips or from contaminated soil brought in from outside. Pottery. Glazes found on some ceramics, china and porcelain can contain lead that can leach into food served or stored in the pottery. Toys. Lead is sometimes found in toys and other products produced abroad. Cosmetics. Tiro, an eye cosmetic from Nigeria, has been linked to lead poisoning. Herbal or folk remedies. Lead poisoning has been linked to greta and azarcon, traditional Hispanic medicines, as well as some from India, China and other countries. Mexican candy. Tamarind, an ingredient used in some candies made in Mexico, might contain lead. Lead bullets. Time spent at firing ranges can lead to exposure. Occupations. People are exposed to lead and can bring it home on their clothes when they work in auto repair, mining, pipe fitting, battery manufacturing, painting, construction and certain other fields
