Top Videos
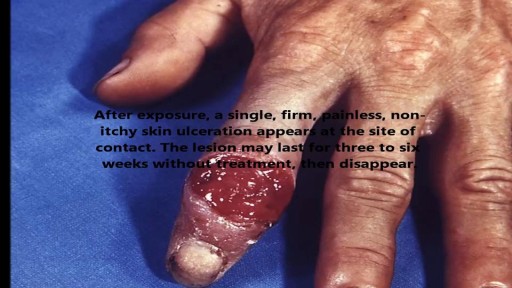
STDs are infections that are transmitted during vaginal, anal, and oral sex. They are very common and many people who have them don't show any symptoms.
USMLE Step 2 CS - Shoulder Pain This is just preview video. To get full access please visit our website : www.usmletutoring.com

http://penilepapules.plus101.com/ ----- White Spots On Shaft, Pearly Penile Papules Treatment Cream, Single Red Bump On Shaft, Ppp Surgery. Common Home Made Remedies for Pearly Penile Papules. When it comes to treating pearly penile papules many people find it very difficult to reach one of the medical treatments. This is mainly because they are highly expensive and not many people can afford spending large amounts of money on surgery and recovery. In addition to that, these procedures have been reported as being quite risky, which make the men suffering from pearly penile papules think twice before going for one of the available surgeries. This is why, along the time, many homemade, natural treatments have been experienced, so that a cheaper and less risky way of curing pearly penile papules would be found. Some of the methods which have been tried proved to be very less effective, while some did not have any effect at all. Yet, there have also been methods which not only proved to be effective, but they were also considered to be much better than the medical treatment. Most of those who have tried the tea tree oil treatment reported significant diminish of the number of the papules from their penises. In addition to the clearing of the skin, they have also noticed that there were no side effects and the skin remained soft after the papules were removed. As the method was quite simple to put in practice (it requires the application of tea tree oil on the affected area with a cotton swab for three or four times per day), many men decided this was indeed a great solution to their problem.

Dr. Linder is removing a patients breast implants after having five breast augmentations from three previous surgeons. She has baker 4 capsular contracture and is look forward to having them removed. The most common reasons for removing a breast implant include; heath reasons such as back pain, reoccurring complications and the desire for a different shape or size. For implant removal surgery, Dr. Linder makes an inframammary incision (along the breast crease). The implant can be removed intact, or it may need to be punctured before removal. An antibiotic solution is used to irrigate the breast pocket after implant removal. For more information about breast implant removal go to www.implantremoval.net or call Dr. Linder's office at 310-275-4513

The Talizi Hair Transplantation Clinic offers hair restoration through a painless hair transplantation procedure and guarantees a natural result for an affordable price. 6000 grafts at one session. Hair transplantation surgery combining seamless Follicular Unit Extraction FUE method and Strip Version.

In this video I show the steps to give a woman a full body energy orgasm without even touching her.
Pleurisy is a condition in which the pleura — a membrane consisting of a layer of tissue that lines the inner side of the chest cavity and a layer of tissue that surrounds the lungs — becomes inflamed. Also called pleuritis, pleurisy causes sharp chest pain (pleuritic pain) that worsens during breathing. A variety of underlying conditions can cause pleurisy. Treatment of pleurisy involves pain control and treating the underlying condition.

Bleeding usually occurs from only one nostril. If the bleeding is heavy enough, the blood can fill up the nostril on the affected side and overflow within the nasopharynx (the area inside the nose where the two nostrils merge), spilling into the other nostril to cause bleeding from both sides. Blood can also drip back into the throat or down into the stomach, causing a person to spit or even vomit blood. Signs of excessive blood loss include dizziness, light-headedness, confusion, and fainting. Excessive blood loss from nosebleeds is rare. Additional bleeding from other parts of the body, such as bleeding gums when brushing teeth, blood in urine or bowel movements, or easy bruising may indicate an inability of the blood to clot. Additional bleeding or easy bruising can be a sign of a more significant medical problem.

Use warm water and sea salt. Soak the wart for 10 to 15 minutes in warm salt water to moisten the skin. Scrape the dead skin layers off the wart using a nail file, pumice stone or mild sandpaper. You could also use your fingers, but wash them thoroughly before and after, as warts can easily spread.

A video showing the procedure of lipoma excision

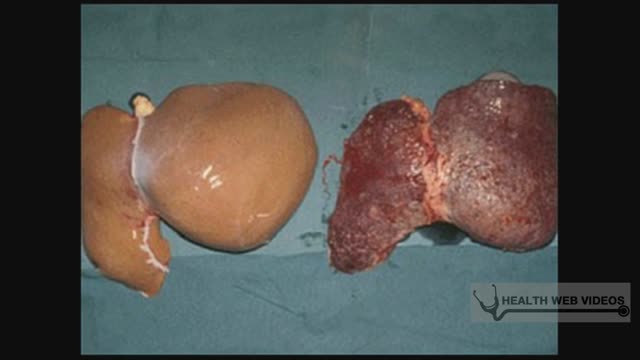
Hepatitis A is a highly contagious liver infection caused by the hepatitis A virus. The virus is one of several types of hepatitis viruses that cause inflammation and affect your liver's ability to function. You're most likely to contract hepatitis A from contaminated food or water or from close contact with someone who's infected. Mild cases of hepatitis A don't require treatment, and most people who are infected recover completely with no permanent liver damage. Practicing good hygiene, including washing hands frequently, is one of the best ways to protect against hepatitis A. Vaccines are available for people most at risk.


Dentist Kennewick WA Call (509) 783-8822

http://www.pearlywhiteslv.com
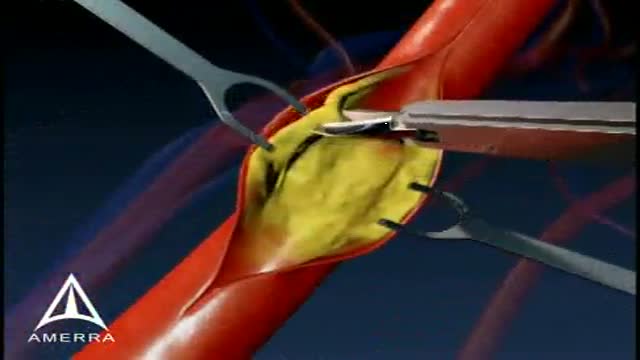
This medical animation is aimed at educating patients about the basics of a Carotid Endarectomy.

Management of postpartum hemorrhage at vaginal delivery. The approach to treatment of postpartum hemorrhage (PPH) differs somewhat depending on the cause and whether hemorrhage occurs after a vaginal birth or after a cesarean delivery.

Initial symptoms may include: Pain or discomfort in the upper tummy (abdomen), especially after eating. Indigestion. (Note: most people who have indigestion do not have stomach cancer.) Feeling sick, and being off food. ... Weight loss and/or loss of appetite. You may pass blood out with your stools (faeces).
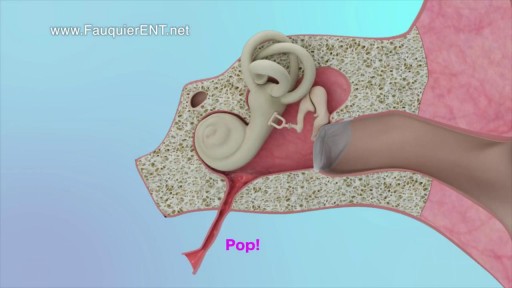
This video demonstrates why ears become clogged and why ear popping helps. The video also explains why ear popping may become difficult resulting in a persistent clogged or muffled ear especially after an ear infection.
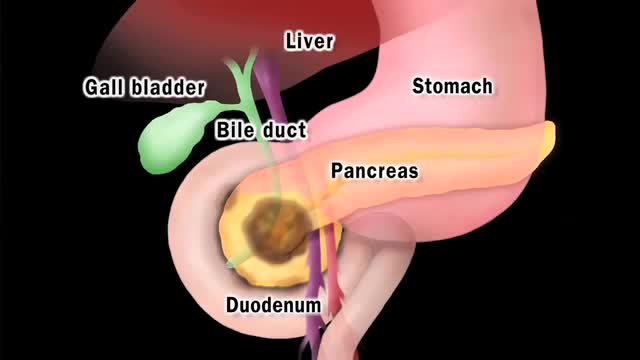
Pancreatic cancer begins in the tissues of your pancreas — an organ in your abdomen that lies horizontally behind the lower part of your stomach. Your pancreas secretes enzymes that aid digestion and hormones that help regulate the metabolism of sugars. Pancreatic cancer often has a poor prognosis, even when diagnosed early. Pancreatic cancer typically spreads rapidly and is seldom detected in its early stages, which is a major reason why it's a leading cause of cancer death. Signs and symptoms may not appear until pancreatic cancer is quite advanced and complete surgical removal isn't possible.
