- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Nose Cyst Extraction
Open heart (coronary artery bypass, or CABG) surgery is performed in order to reroute, or "bypass," blood around blocked arteries, thereby improving the supply of oxygen-rich blood to the heart. Surgeons usually use an artery from the chest wall to construct the "detour" around the blocked part of the artery. Veins from the legs are also used.

Gastric bypass, also called Roux-en-Y gastric bypass surgery, is considered a “metabolic” procedure because it changes how your body absorbs fat, calories and nutrients. This metabolic change occurs because your gastrointestinal tract is altered when your gastric bypass surgeon attaches the smaller section of your stomach directly to your small intestine. As a result, your appetite changes and you feel full faster.
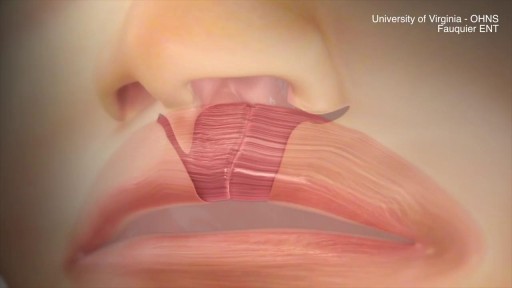
This animation demonstrates how a unilateral complete cleft lip repair is performed. This video is meant for educational purposes for patients and families. There are many ways to fix a complete cleft lip, but the technique shown here is the most common known as the Millard Rotation Advancement Repair.

Sprains and Strains

Baby CPR
Kawasaki disease is a condition that causes inflammation in the walls of medium-sized arteries throughout the body, including the coronary arteries, which supply blood to the heart muscle. Kawasaki disease is also called mucocutaneous lymph node syndrome because it also affects lymph nodes, skin, and the mucous membranes inside the mouth, nose and throat. Signs of Kawasaki disease, such as a high fever and peeling skin, can be frightening. The good news is that Kawasaki disease is usually treatable, and most children recover from Kawasaki disease without serious problems.

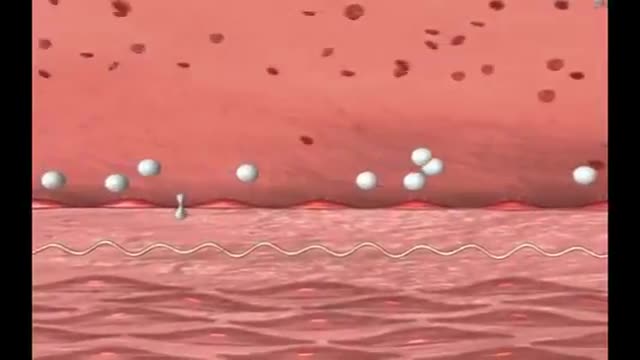
A pulmonary embolism (PE) usually happens when a blood clot called a deep vein thrombosis (DVT), often in your leg, travels to your lungs and blocks a blood vessel. That leads to low oxygen levels in your blood. It can damage the lung and other organs and cause heart failure, too. A PE can be life-threatening, so if you've been diagnosed with DVT, you should be aware of this risk. Follow the treatment plan for your DVT to stop the clot from getting bigger and to keep new clots from forming. Symptoms and Diagnosis PE won't always cause symptoms. You might have: Chest pain, which may get worse with a deep breath Sudden shortness of breath or rapid breathing Fast heartbeat Sudden cough Coughing up blood Lightheadedness or fainting Anxiety Call 911 if you notice these symptoms. They could also be symptoms of a heart attack, pneumonia, or other serious problems.

The common obsession among men and women of having a perfect body has lead them to many serious neurotic disorders. They are constantly exposed to the ideas of having the perfect body. We are bombarded with the images on social media which create a hype among men and women, to achieve the exact same ratio of fats in them. Body image is merely an image of your thoughts and perceptions. The way you think how people notices you can greatly impact yourself and your way of thinking about yourself. It becomes quite a big deal when you start to feel low about yourself. It leads you towards having a low self esteem and it becomes hard for you to feel worthy and confident. On contrary when you have good self esteem you feel empowered and confident. It is not the consequence of just liking your own body but its about accepting who you are and making people accept you as you are.

You might not notice signs or symptoms of Hashimoto's disease at first, or you may notice a swelling at the front of your throat (goiter). Hashimoto's disease typically progresses slowly over years and causes chronic thyroid damage, leading to a drop in thyroid hormone levels in your blood. The signs and symptoms are mainly those of an underactive thyroid gland (hypothyroidism). Signs and symptoms of hypothyroidism include: Fatigue and sluggishness Increased sensitivity to cold Constipation Pale, dry skin A puffy face Hoarse voice Unexplained weight gain — occurring infrequently and rarely exceeding 10 to 20 pounds, most of which is fluid Muscle aches, tenderness and stiffness, especially in your shoulders and hips Pain and stiffness in your joints and swelling in your knees or the small joints in your hands and feet Muscle weakness, especially in your lower extremities Excessive or prolonged menstrual bleeding (menorrhagia) Depression
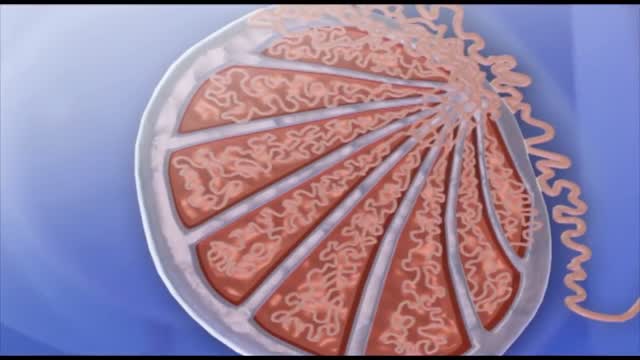
Spermatogenesis is the process in which spermatozoa are produced from spermatogonial stem cells by way of mitosis and meiosis. The initial cells in this pathway are called spermatogonia, which yield primary spermatocytes by mitosis.
Gitelman syndrome is a kidney disorder that causes an imbalance of charged atoms (ions) in the body, including ions of potassium, magnesium, and calcium. The signs and symptoms of Gitelman syndrome usually appear in late childhood or adolescence. Common features of this condition include painful muscle spasms (tetany), muscle weakness or cramping, dizziness, and salt craving. Also common is a tingling or prickly sensation in the skin (paresthesias), most often affecting the face. Some individuals with Gitelman syndrome experience excessive tiredness (fatigue), low blood pressure, and a painful joint condition called chondrocalcinosis. Studies suggest that Gitelman syndrome may also increase the risk of a potentially dangerous abnormal heart rhythm called ventricular arrhythmia. The signs and symptoms of Gitelman syndrome vary widely, even among affected members of the same family. Most people with this condition have relatively mild symptoms, although affected individuals with severe muscle cramping, paralysis, and slow growth have been reported.

Clogged leg arteries can be opened through a minimally invasive procedure with the SILVERHAWK, a mini drill with a tiny rotating blade for cutting away plaque. The procedure only involves a tiny puncture in the patient's groin. ~ Detroit Medical Center

This video shows the delivery of the placenta after delivery of the fetus

The timing of the nausea or vomiting can indicate the cause. When appearing shortly after a meal, nausea or vomiting may be caused by food poisoning, gastritis (inflammation of the stomach lining), an ulcer, or bulimia. Nausea or vomiting one to eight hours after a meal may also indicate food poisoning.
Trichinosis (trik-ih-NO-sis), sometimes called trichinellosis (trik-ih-nuh-LOW-sis), is a type of roundworm infection. Roundworm parasites use a host body to live and reproduce. Occurring primarily among meat-eating animals (carnivores) — especially bears, foxes and walruses — the infection is acquired by eating roundworm larvae in raw or undercooked meat. When humans eat undercooked meat containing trichinella larvae, the larvae mature into adult worms in the intestine over several weeks. The adult worms then produce larvae that travel through various tissues, including muscle. Trichinosis is most widespread in rural areas throughout the world. Trichinosis can be treated with medication, though it's not always necessary. It's also easy to prevent.
LASER SURGERY Pilonidal Cyst removal

Anterior Release Test

During 34 week of pregnancy, the baby is getting ready for delivery, you may feel less wriggling and kicking. Watch out this video to learn more about being 34 weeks pregnant.

Emergency C Section for a Bleeding Placenta
