- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Visit our website to learn more about using Nucleus content for patient engagement and content marketing: http://www.nucleushealth.com/
#LaparoscopicColectomy #ColonSurgery #LargeIntestine
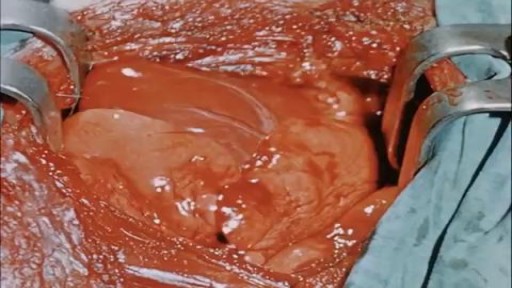
A colectomy is usually done to treat diseases that inflame your colon, a bowel obstruction, colon cancer, or a damaged or injured colon. The anatomy of the colon, and the laparoscopic procedure done to remove a portion of the colon, are depicted.
ANH18221

A Cesarean section (C-section) is surgery to deliver a baby. The baby is taken out through the mother's abdomen. In the United States, almost one in three women has their babies this way. Some C-sections are planned, but many are done when unexpected problems happen during delivery. Reasons for a C-section may include Health problems in the mother The mother carrying more than one baby The size or position of the baby The baby's health is in danger Labor is not moving along as it should
A report of Female Genital Mutilationn FGM (female circucision) in Menya In Egypt تقرير من مدينة المنيا في صعيد مصر عن ختان لاناث

This is a diabetic foot ulcer. The patient reportedly went on vacation and noticed this ulcer upon their return. Debridement (removal of damaged tissue) to the level of healthy bleeding tissue is medically necessary as damaged tissue acts an impediment to wound healing. Due to their diabetic neuropathy, they did not feel any pain or indication that a wound was forming. This ulcer appeared to have penetrated to the level of subcutaneous tissue or even fascia, but turned out to be much deeper than that. These are serious wounds and are the beginnings of what lead to foot and leg amputations if they are not treated promptly by your healthcare provider, AKA Podiatrist.

Watch that Baby Abortion Medical Procedure
Vaginal discharge serves an important housekeeping function in the female reproductive system. Fluid made by glands inside the vagina and cervix carries away dead cells and bacteria. This keeps the vagina clean and helps prevent infection. Most of the time, vaginal discharge is perfectly normal. The amount can vary, as can odor and hue (its color can range from clear to a milky white-ish), depending on the time in your menstrual cycle. For example, there will be more discharge if you are ovulating, breastfeeding, or are sexually aroused. The smell may be different if you are pregnant or you haven't been diligent about your personal hygiene. None of those changes is cause for alarm. However, if the color, smell, or consistency seems significantly unusual, especially if it accompanied by vaginal itching or burning, you could be noticing an infection or other condition. What causes abnormal discharge? Any change in the vagina's balance of normal bacteria can affect the smell, color, or discharge texture. These are a few of the things that can upset that balance:

Childbirth (also called labour, birth, partus or parturition) is the culmination of a human pregnancy or gestation period with the birth of one or more newborn infants from a woman's uterus. The process of normal human childbirth is categorized in three stages of labour: the shortening and dilation of the cervix, descent and birth of the infant, and birth of the placenta. In many cases, with increasing frequency, childbirth is achieved through caesarean section, the removal of the neonate through a surgical incision in the abdomen, rather than through vaginal birth. In the U.S. and Canada it represents nearly 1 in 3 (31.8%) and 1 in 4 (22.5%) of all childbirths, respectively.
Full examination of the female from head to toe by Loyola Medical School, Chicago part 1

exam

Laser tattoo removal is simple, safe, and produces fantastic...

A spontaneous vaginal delivery (SVD) occurs when a pregnant woman goes into labor with or without use of drugs or techniques to induce labor, and delivers her baby in the normal manner, without forceps, vacuum extraction, or a cesarean section. Assisted vaginal delivery (AVD) occurs when a pregnant woman goes into labor with or without the use of drugs or techniques to induce labor, and requires the use of special instruments such as forceps or a vacuum extractor to deliver her baby vaginally.

An abdominal hysterectomy is a surgical procedure that removes your uterus through an incision in your lower abdomen. Your uterus — or womb — is where a baby grows if you're pregnant. A partial hysterectomy removes just the uterus, leaving the cervix intact. A total hysterectomy removes the uterus and the cervix. Sometimes a hysterectomy includes removal of one or both ovaries and fallopian tubes, a procedure called a total hysterectomy with salpingo-oophorectomy (sal-ping-go-o-of-uh-REK-tuh-me). A hysterectomy can also be performed through an incision in the vagina (vaginal hysterectomy) or by a laparoscopic or robotic surgical approach — which uses long, thin instruments passed through small abdominal incisions.
Are you a first time would be mom? If yes, then you must be very excited to feel the first movement and kick from your baby. It is undoubtedly the most exciting experience for many expecting moms. It is an indication that there is a little angel growing inside you. There are interesting facts about baby kicks during pregnancy that you need to know.
The treatment of cardiac arrest

A video showing the process of childbirth via vaginal delivery.

This video - produced by students at Oxford University Medical School - demonstrates how to perform an examination of the respiratory system. It also indicates common pathologies encountered. It is part of a series of videos covering basic clinical examinations and is linked to Oxford Medical Education (www.oxfordmedicaleducation.com).

Debridement of an Infected Diabetic Wound on the patients foot. The first is a series of online diabetic foot care videos by The Mayer Institute. Themayerinstitute.ca

A video discussing Causes of Itching in the Vulva

Watch that video to know if it is safe to have sex during pregnancy
